Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191101_004
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Left Main Bifurcation: What and How? | |
| Shahab Uddin Talukder1, Mahmood Hasan Khan | |
| Evercare Hospital Dhaka, Bangladesh1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. RK
-Relevant clinical history and physical exam:
•RK •Age: 62 years •Gender: Male •Risk Factors: Dyslipidemia, Positive Family history of CAD. •Complaining mainly of effort angina (Class II/III) for a few months now. •ECG: OMI (Ant-Sept) •Echo: RWMA (+) with LVEF: 45% •H/O Primary PCI to LAD & PCI to OM. 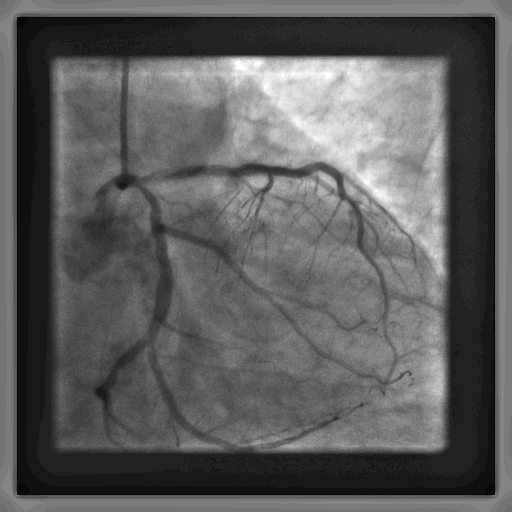   -Relevant test results prior to catheterization:
Hemoglobin: 13.8 gm/dl TLC: 8.77 x 109/L Platelet: 208 x 109/L Creatinine: 1.10 mg/dl Na: 135 mmol/L K: 4.2 mmol/L 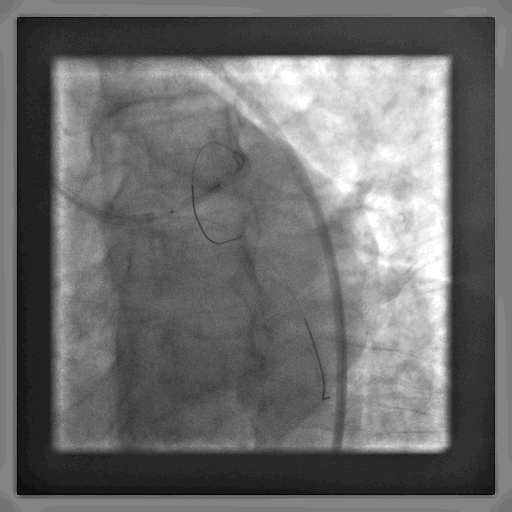 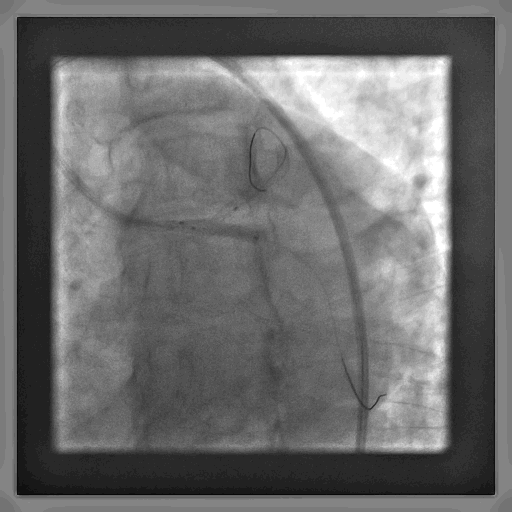 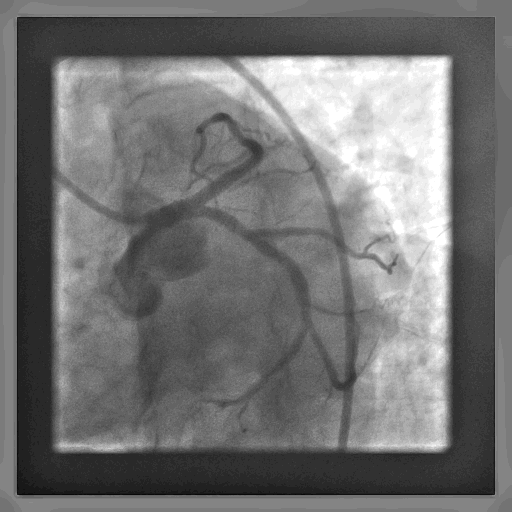 - Relevant catheterization findings:
CAD -SVD with ISR in LAD Patent stent in OM Recommendation: PCI to LM - LAD & LCx / CABG.Syntax I score: 18.
•Route Used: Right Femoral •Guide Catheter: JL 3.5 7F •Guide Wires: Floppy (x 2) •Balloons: 2.0x15 mm & 3.0x10 mm for pre-dilation 4.5x10 mm (x 2) forpost-dilationStents Used:•4.0 mm x 23 mm DES for LM - LAD •3.5 mm x 15 mm DES for LCx |
|
|
[Interventional Management]
- Procedural step:
Wiring of the culprit lesion with floppy wires
Pre- dilation of the lesions with 2.0 x 15 mm and 3.0 x 15 mm balloons. First KISS Positioning& deployment of LCx stent. First Crush LM-LAD stent positioning & deployment Second Crush Second KISS Re-wiring & POT… IVUS assessment Final Cine •Mandatory when using a two- stent strategy. •Provides significant reduction in MB & SB re-stenosis. •Must be performed optimally using appropriately sized balloons: –Sequential high-pressure balloon dilatation of the SB stent then the MB stent. –Finalize with lower pressure kissing balloon dilatation. 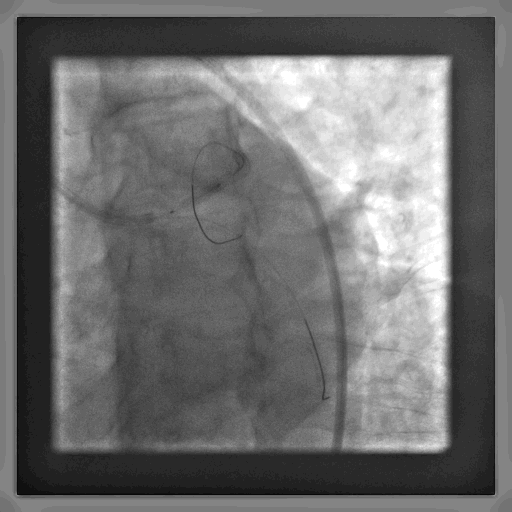 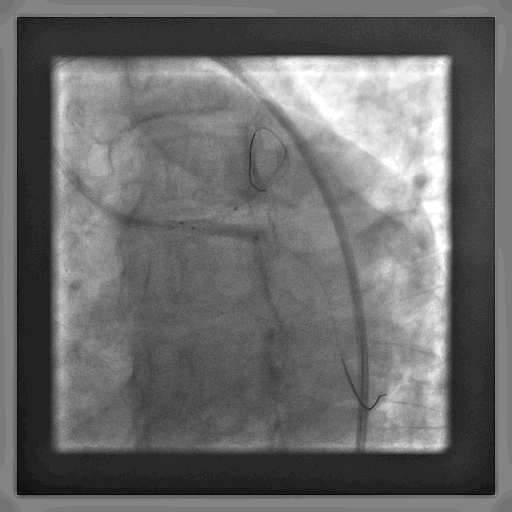 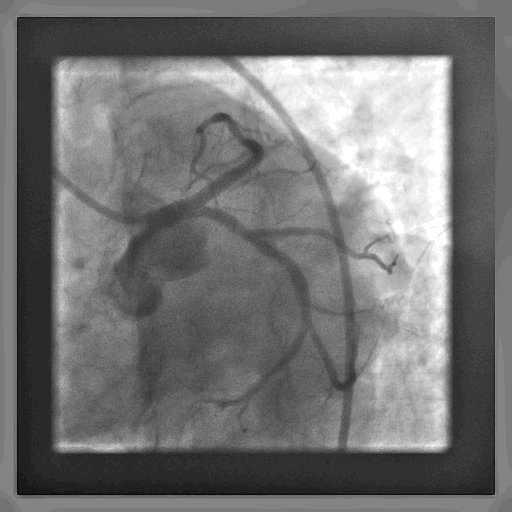 - Case Summary:
•Mandatory when using a two-stent strategy. •Provides significant reduction in MB & SB re-stenosis. •Must be performed optimally using appropriately sized balloons: –Sequential high-pressure balloon dilatation of the SB stent then the MB stent. –Finalize with lower pressure kissing balloon dilatation. •DK Crush technique is the preferred technique. •We wire the SB twice. •We KISS twice! •POT is essential. •IVUS guidance is mandatory when treating Complex LM & non – LM bifurcation lesions. •IVUS guidance leads to lower MACE rates lead by decreased rates of stent thrombosis& target lesion revascularization. |
|