Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_048
| CORONARY - Chronic Total Occlusion | |
| A Coronary Marathon | |
| Lap Ti Lam1 | |
| Grantham Hospital, Hong Kong, China1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Ma
-Relevant clinical history and physical exam:
A 75 years old man had past medical history of type II diabetes mellitus, hyperlipidemia and atrial fibrillation. He received coronary artery bypass graft surgery 20 years ago. The bypass surgery involved a LIMA to LAD and SVG to RCA/OM/Diagonal branch. He received PCI to SVG of OM branch in 2004 and to proximal left circumflex artery in 2005. Percutaneous coronary intervention to RCA CTO was failed in 2005. He presented with stable effort angina.
-Relevant test results prior to catheterization:
Echocardiogramshowed left ventricular ejection fraction of 45% with anteroseptal wall hypokinesia. The valves were structurally normal.
- Relevant catheterization findings:
Coronary angiogram showed mild left main disease, osital LAD 90% stenosis, blocked mid LAD, patent proximal left circumflex artery stent, mid left circumflex 60% stenosis, blocked distal left circumflexartery, mRCA CTO, retrograde filling from LAD and LIMA, patent LIMA to LAD, patent SVG to OM, blocked SVG to D1 and blocked SVG to RCA.
  |
|
|
[Interventional Management]
- Procedural step:
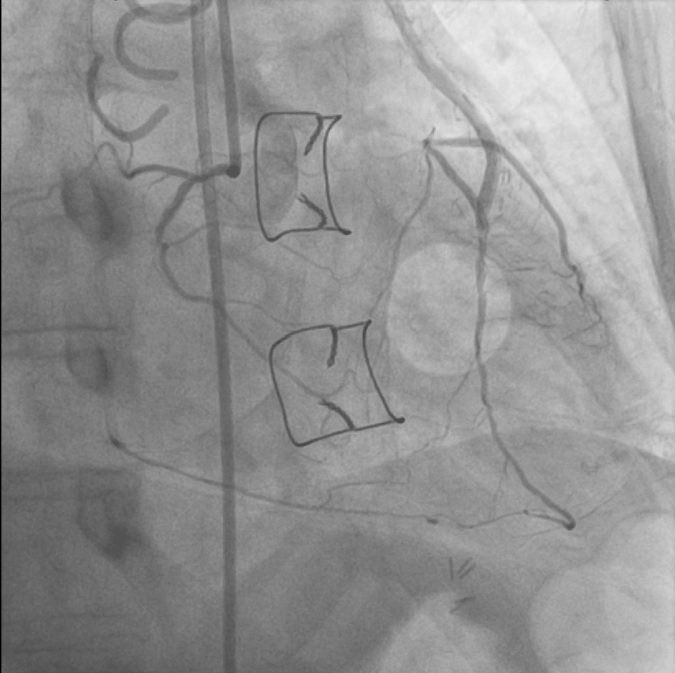
The RCA was engaged with a 7Fr JR4 guiding catheter via right radial artery and the LIMA was engaged with a 90cm 7Fr IMA guiding catheter via right femoral artery. The proximal cap of the mid RCA CTO was crossed by Fielder XT supported by Corsair Microcatheter. However, the FielderXT easily went into side branch. Parallel wiring using Gaia 2 supported by Crusade failed to advance across the CTO body. Therefore, the strategy was switched to retrograde approach. The septal channel from LIMA was crossed with Sion wire supported by 150cm Corsair microcatheter. Then the retrograde wire was changed to Fielder XTR which allowed further advancement across the distal cap of CTO. However, the Corsair catheter was too short to advance up to mid RCACTO body. Then, further antegrade preparation was performed. A 6Fr GuideLiner was placed at the proximal RCA after 2.5/15 balloon dilatation. Furthermore, the IMA guiding catheter was deeply intubated into LIMA. The fielder XT wire was changed Gaia 2nd wire. Finally, the Gaia 2nd wire and Corsair microcatheter could advance into the GuideLiner. The Gaia 2nd was exchanged to RG3 and externalized. IVUS was used to confirm the position of the wire. Despite serial dilatation of the RCA with non-compliant balloon, cutting balloon or OPN balloon, the drug eluting stent could not be delivered with the support of 7Fr GuideLiner. Afterwards, the whole RCA was modified with Rotablator 1.75 burr. Finally the RCA was successfully stented with three DES.
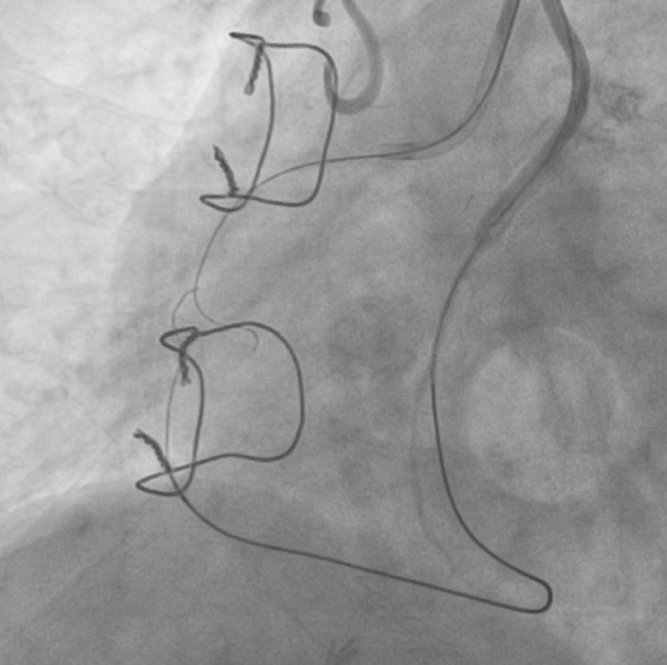 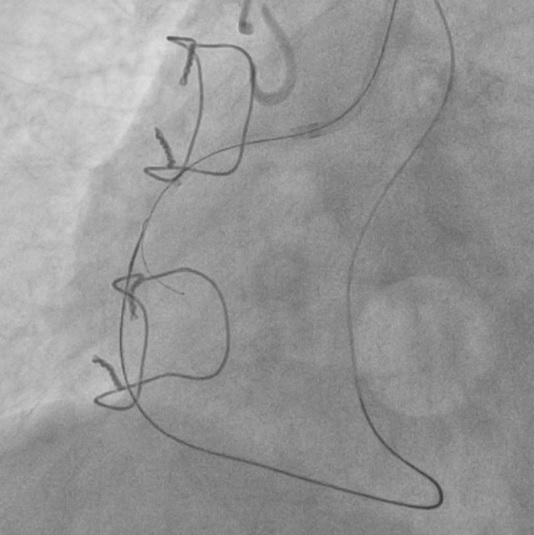 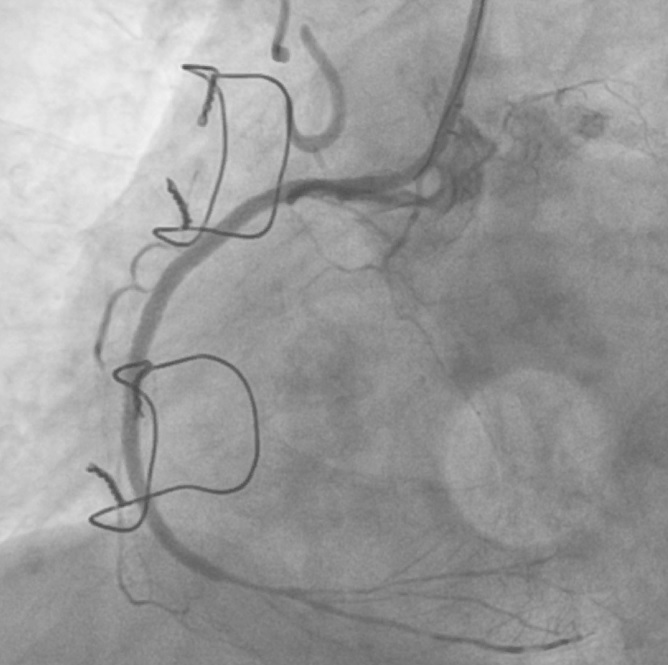 - Case Summary:
It is challenging to treat RCA CTO using LIMA-septal retrograde channel. The long-distance retrograde wiring is one of the most difficult parts to deal with. It may reduce the chance of procedure success. This case illustrated the ways to overcome this problem including the use of short guiding catheter with deep intubation, use of long microcatheter and antegrade preparation with GuideLiner.
|
|