Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_046
| CORONARY - Complications | |
| Iatrogenic Left Main Coronary Artery Obstruction After Aortic Valve Replacement | |
| Kuo Wei Chung1, Chiate Liao2 | |
| Chi Mei Hospital Liouying, Taiwan1, Chi Mei Medical Center, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
13966552
-Relevant clinical history and physical exam:
A 76-year-old woman presented to our cardiovascular clinic due to the progressive shortness of breath resulted from severe aortic stenosis (AS) and mitral stenosis (MS). After the pre-surgery evaluation, double valve replacement was smoothly performed. However, after the surgery, this patient intermittently had the sensation of chest compression.
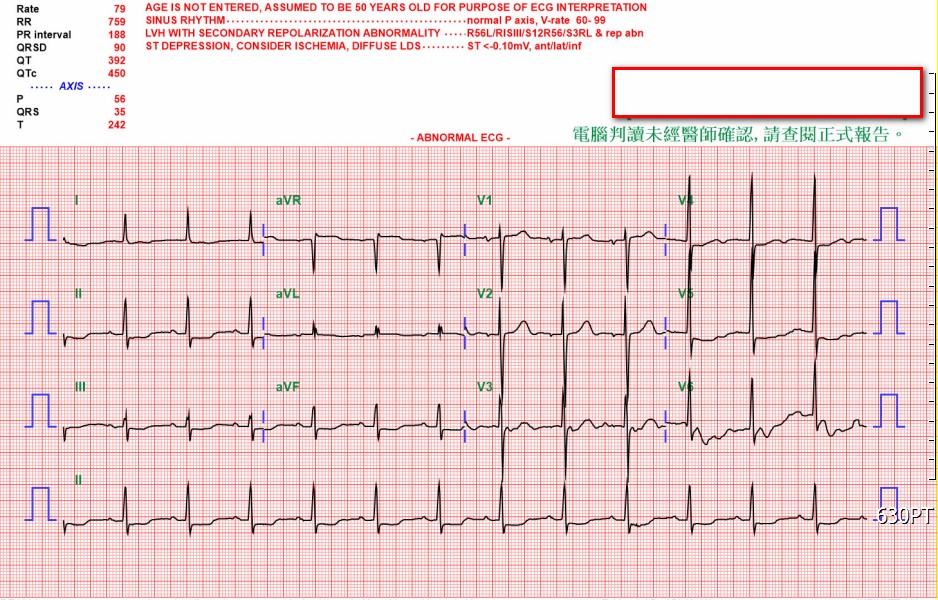
 -Relevant test results prior to catheterization:
ECG was arranged and it disclosed insignificant ST segment elevation in lead aVR, accompanied by ST segment depression in leads II, III, aVF, V4, V5, and V6. Furthermore,the following ECG showed new-onset right bundle branch block, and cardiac enzymes elevated. Meanwhile, echocardiography revealed that left ventricle ejection fraction (LVEF) deteriorated from 63% to 26%, comparing the previous one before two months.
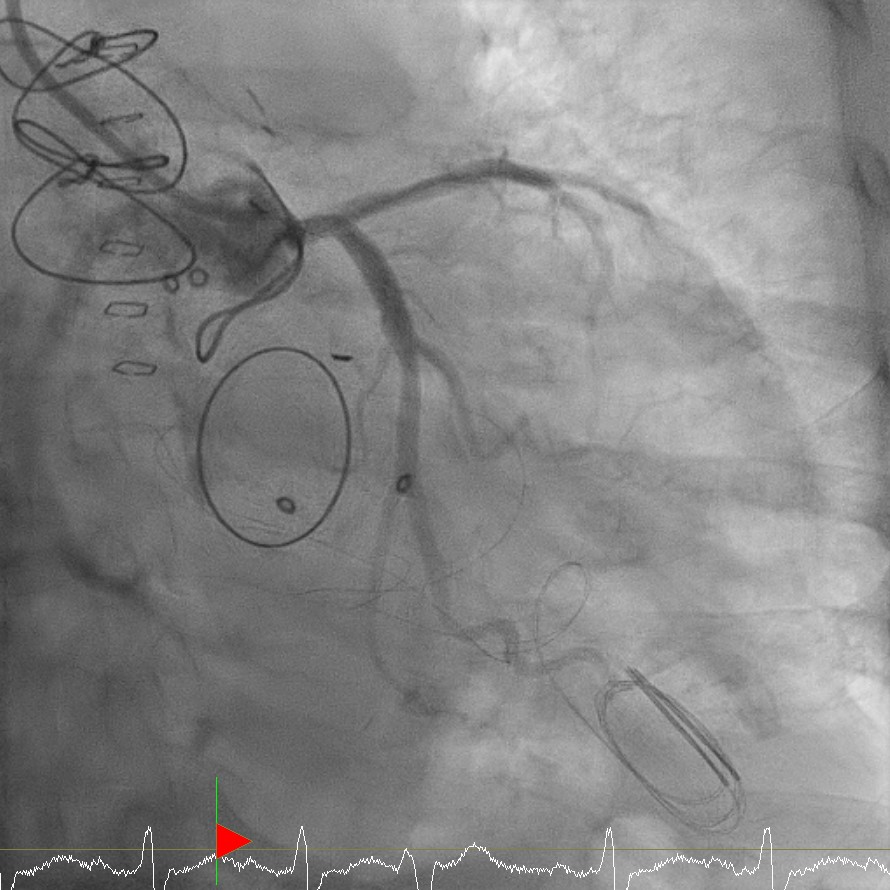
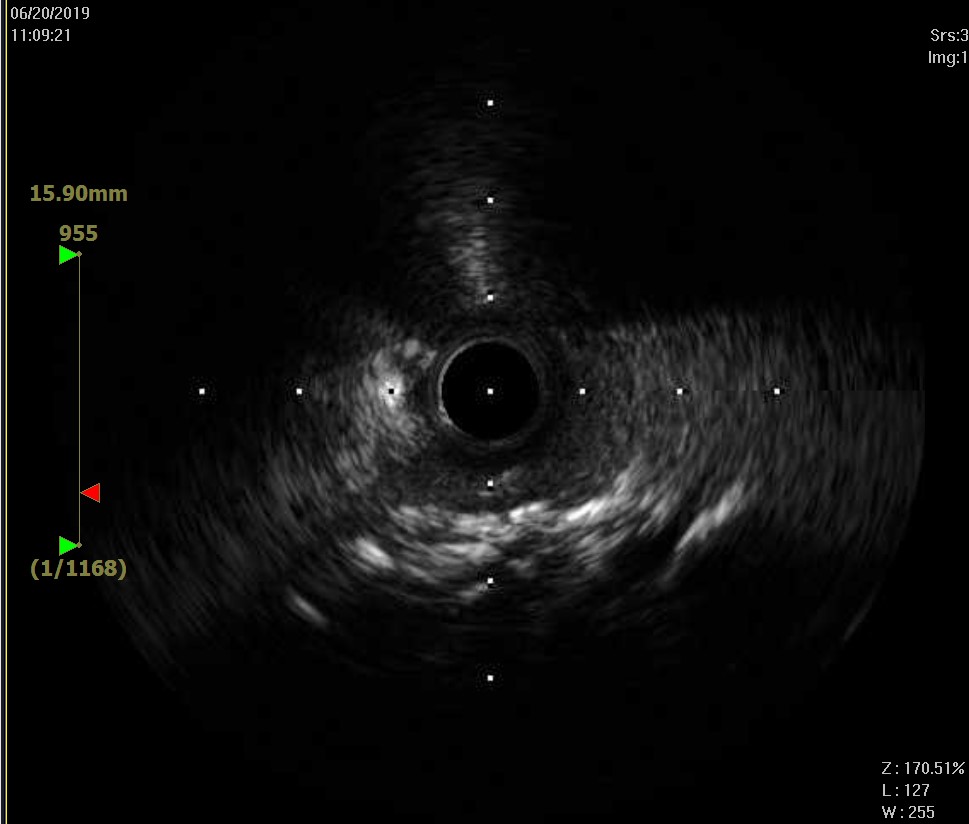
 - Relevant catheterization findings:
From the coronary angiogram, coronary arteries were radiologically patent, while the LMCA ostium was obstructed by a heterogenous lesion, like the AVR suture line and the ring of artificial valve. To assess the lesion, the intravascular ultrasound (IVUS) was utilized and it revealed that the orifice was mechanically compressed by the foreign tissue.
  |
|
|
[Interventional Management]
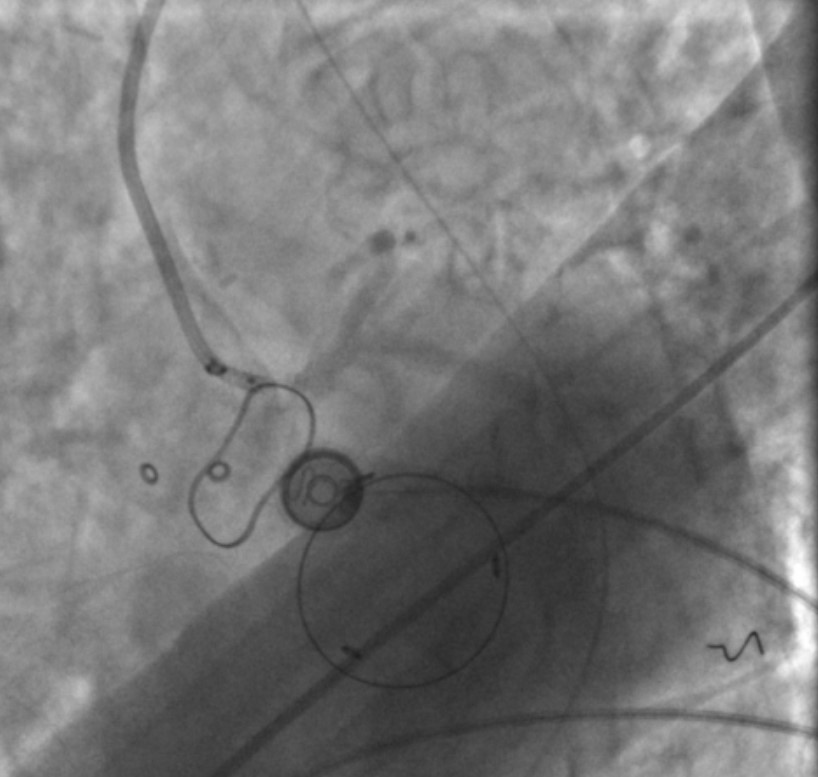
- Procedural step:
We performed several times of plain old balloon angioplasty (POBA) with Maverick 4.0x12mm up to 16 ATM to dilate the obstructive LMCA ostium. However, the compression strength was likely too strong to totally restore the LMCA ostium flow. Therefore, we deployed a bare metal stent REBEL 4.5x12mm up to 14 ATM, and afterward we used a high-pressure balloon for post-stenting dilatation (NC Emerge 5.0x 8mm, up to 16 ATM). Despite the repeated dilatation and total expansion of the high-pressure balloon, the LMCA orifice recoiled shortly, accompanied by reduced coronary inflow. Due to the refractory recoiling of LMCA orifice, cardiogenic shock, and congestive heart failure, coronary artery bypass graft (CABG) was taken into account for better revascularization. Next day, CABG was carried out and the great saphenous vein graft was anastomosed to the proximal left anterior descending artery with end-to-side fashion. The left circumflex artery was not revascularized because of the previous mitral valve replacement and left ventricular hypertrophy. After CABG, this patient was cared in the ICU. However, in the following management, endotracheal extubation was difficult due to her heart failure and repeated infection. After tracheostomy, she successfully weaned the ventilator. Eventually, she was discharged to nursing home.
 - Case Summary:
Iatrogenic coronary artery ostial obstruction after AVR is an uncommon complication. However, the clinical presentation may range from angina to cardiogenic shock and even death. In order to avoid the complication, the operator should ensure the position of thecoronary artery orifices and avoid they are obstructed after AVR. Once the complicatio nhappens, revascularization should be performed as soon as possible. Give a failed revascularization via PCI, CABG would be an optimal management. In this case report, we deeply hope the experience may help to meliorate the complication and provide a strategy to shoot trouble.
|
|