Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_045
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| Carve Your Way: Orbital Atherectomy with Mechanical Circulatory Support in Severely Calcified Lesions | |
| Tsz Ho Chan1, Yu Ho Chan2 | |
| Pok Oi Hospital, Hong Kong, China1, The CUHK Medical Centre, Hong Kong, China2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Chan
-Relevant clinical history and physical exam:
63 years old gentleman, poor control on diabetes, hypertension, hyperlipidemia and chronic kidney disease, admitted to hospital because of acute pulmonary edema. He was intubated and transferred to our unit. After good diuresis and stabilization, the patient managed to be extubated and planned for revascularization. -Relevant test results prior to catheterization:
Chest x ray showed congested lung fields. Electrocardiogram showed poor R wave progression in anterior leads. Blood test showed raised creatinine and cardiac enzymes. Echocardiogram showed global hypokinesia and ejection fraction less than 35%. 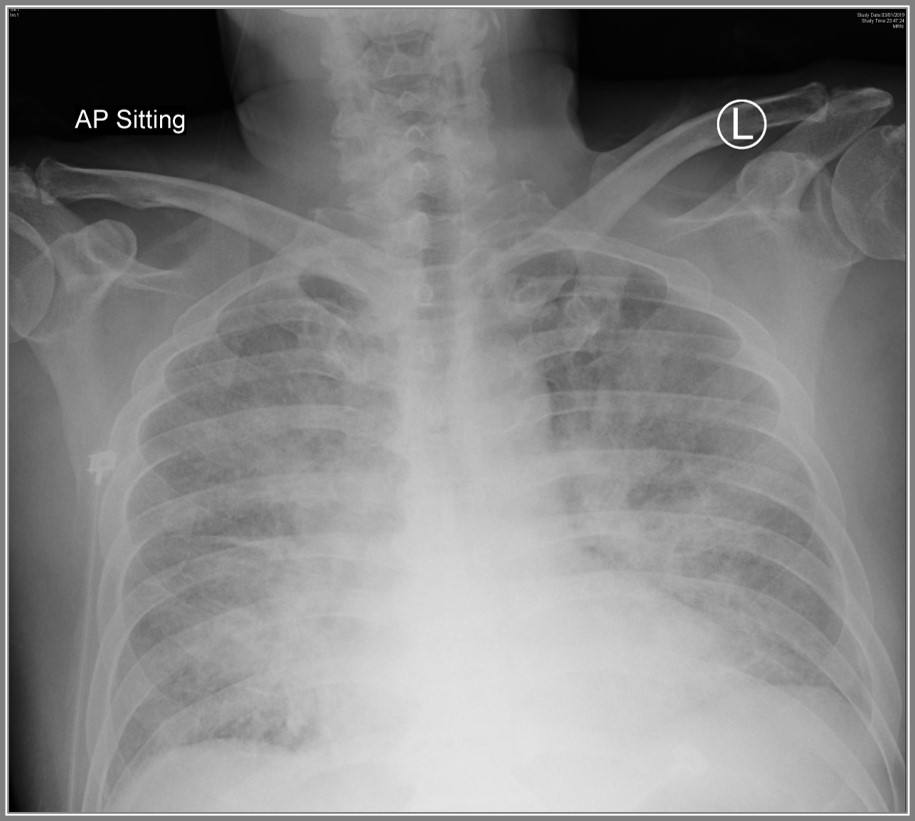 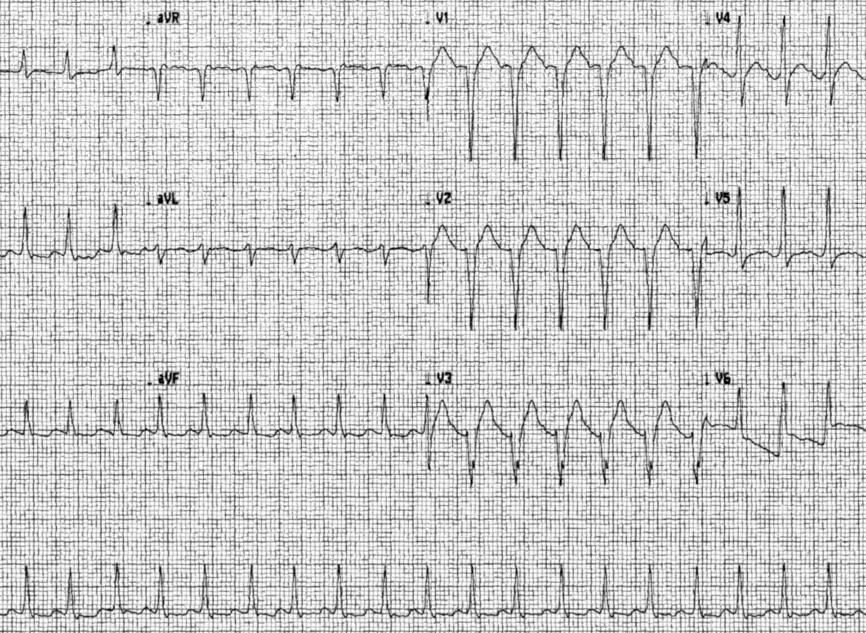 - Relevant catheterization findings:
The diagnostic coronary angiogram showed triple vessels disease, diffuse and heavily calcified lesions.
Left main was normal.Left anterior descending artery (LAD) showed severe 70% over proximal LAD, severe diffuse long 80% proximal to mid LAD, Left circumflex artery (LCx) showed severe 70% mid LCx, subtotal 99% distal LCx with TIMI 1 flow.Right coronary artery showed dominant, severe 80% over posteriolateral branch. 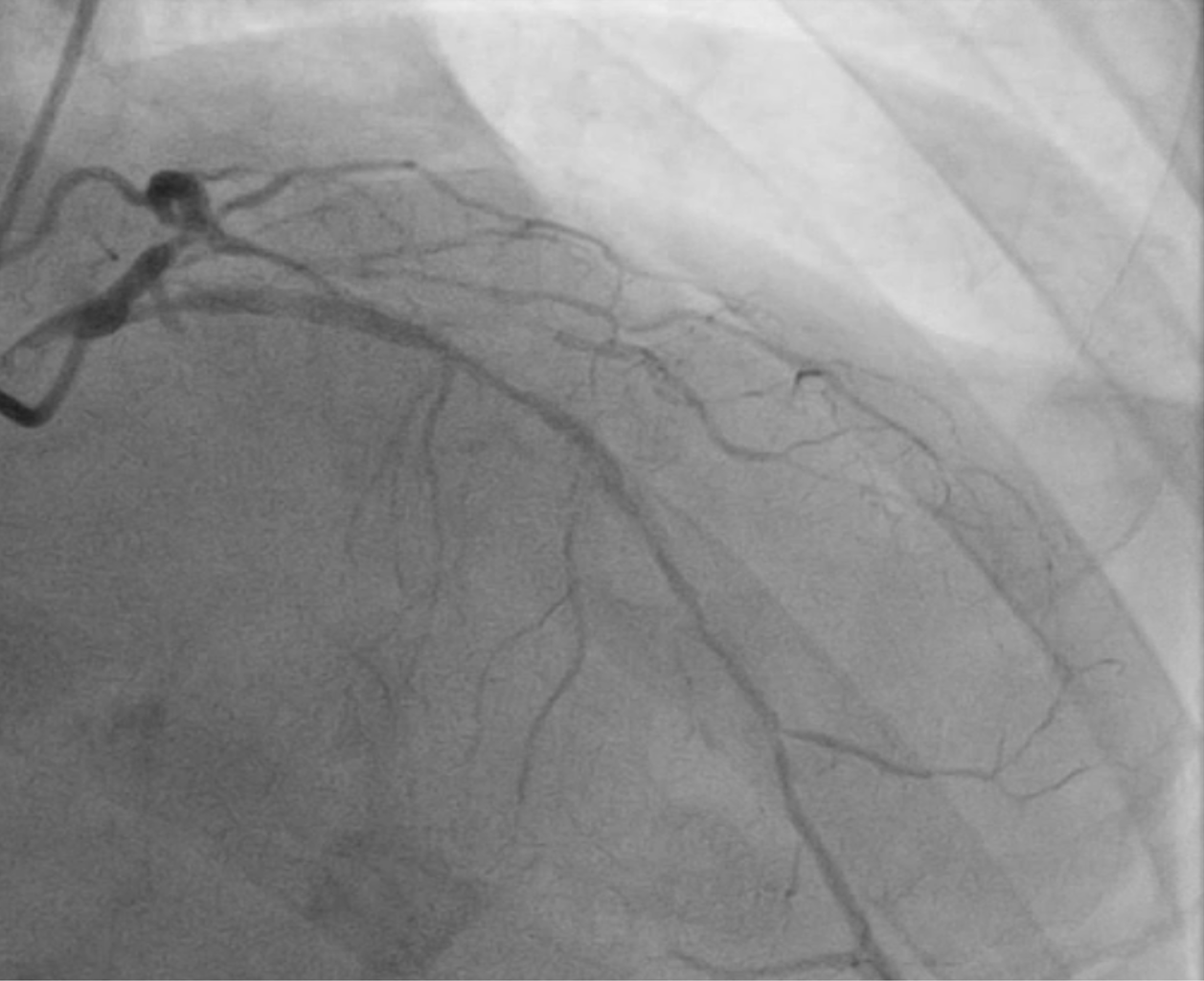  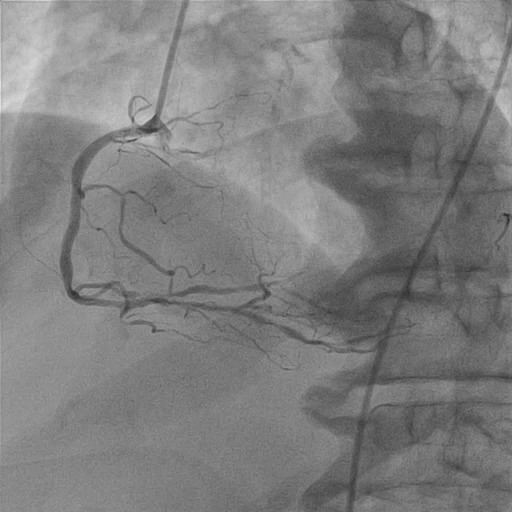 |
|
|
[Interventional Management]
- Procedural step:
Syntax score 1 & 2 were high. Patient strongly refused coronary artery bypass surgery. In view of CHIP case, the patient was first put in Impella Support before PCI through left femoral approach. After having mechanical assist device, we decided to treat the non-culprit lesion (left circumflex artery ) first, then left anterior descending artery. Right coronary artery in view of distal, small branch, planned for medical treatment first and intervention if symptomatic. Left circumflex artery (LCx) lesions were able to be wired by Fielder XT-A with support of Caravel micro-catheter. Calcium plaque is not high but vessel was torturous. Tazuna balloon was used for pre-dilatation. Afterwards stent was deployed and non-compliance balloon was used for post dilatation. TIMI 3 flow achieved. Whole left anterior descending artery (LAD) was heavy calcified. Diamondback given 12 runs in total and lesions pre-dilated by Lacrosse. Afterwards stents were deployed and post dilated by non-compliance balloon. TIMI 3 flow achieved afterwards. No significant change in hemodyanmics seen during procedure. Imeplla was able to be removed at the end of procedure before leaving operation theatre. 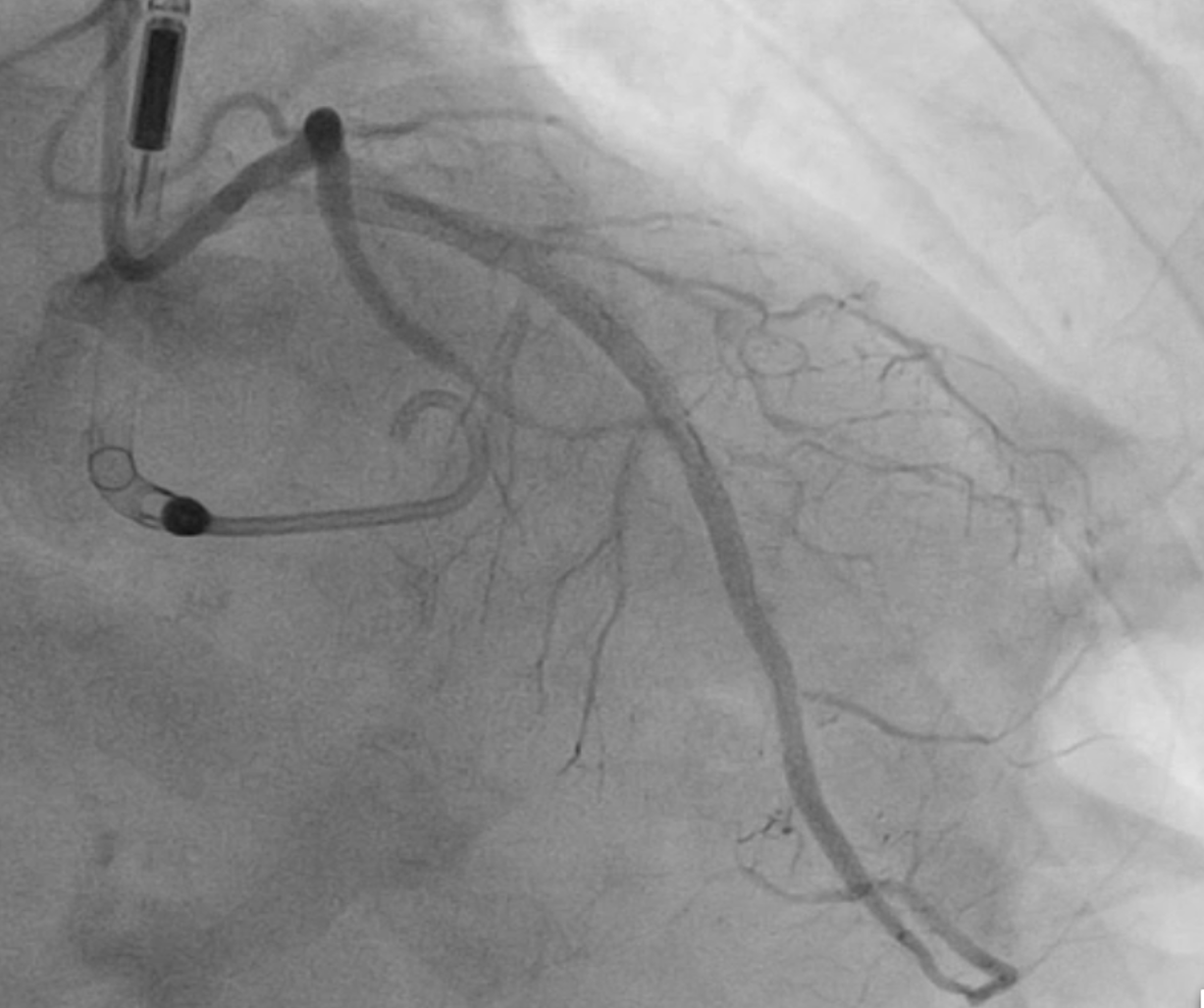 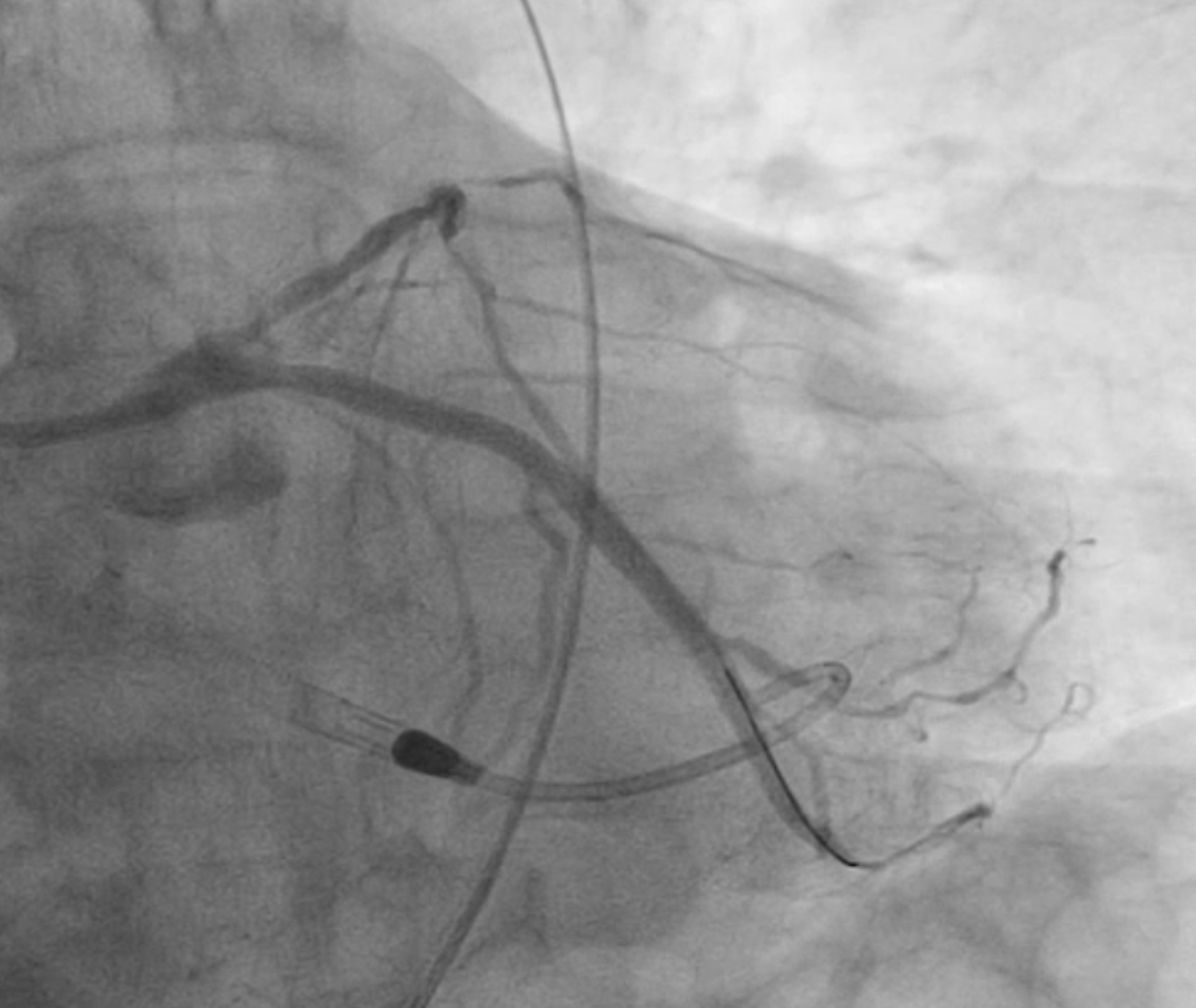 - Case Summary:
CHIP case done under mechanical device support with different difficult lesions with different techniques used in PCI. Discussion points - CHIP definition - Decision on mechanical assist device before intervention. - Mechanical support choices in CHIP - Impella vs other devices. - Different techniques or devices in tackling heavily calcified lesions - orbital or rotational atherectomy, Shockwave. |
|