Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_044
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Acute Myocardial Infarction, RCA Stenosis with Anomalous Left Coronary Artery | |
| Che-Kuang Lin1, Zhih-Cherng Chen2 | |
| Chimei Hospital, Taiwan1, Chi Mei Medical Center, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Y.T Shi
-Relevant clinical history and physical exam:
This 69-year-old male patient who was a smoker about 3-4 pack of cigarettes a day for near 50 years. This time, he suffered from sudden onset of chest tightness during sleeping 30 minutes ago, and accompanied with mild dizziness before arriving emergent room. At ER, electrocardiogram showed no ST-T change, hs-Troponin I elevated (90.00 pg/ml to 8759.00 pg/ml) was found. Under the impression of Non ST Elevation myocardial Infarction, cardiac catheterization was arranged.
-Relevant test results prior to catheterization:
Cardiac angiogram showed 1. CAD, thrombus over RCA, 2. collateral flow from RCA to LAD. Tirofiban (12.5 mg) 13 ml bolus plus iv drip 12 ml/hr for 1 day was given. During the procedure, sustained VT occurred and restored after DC shock200 J. Due to absence of left coronary artery at the cardiac angiogram, we highly suspected LM total occlusion or anomalous left coronary artery. Coronary CTA which showed 1. ectopic left main coronary artery from RCC with malignant course between the LVOT and RVOT.
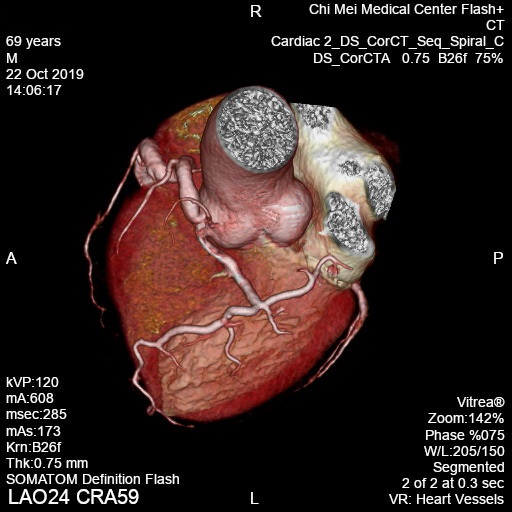 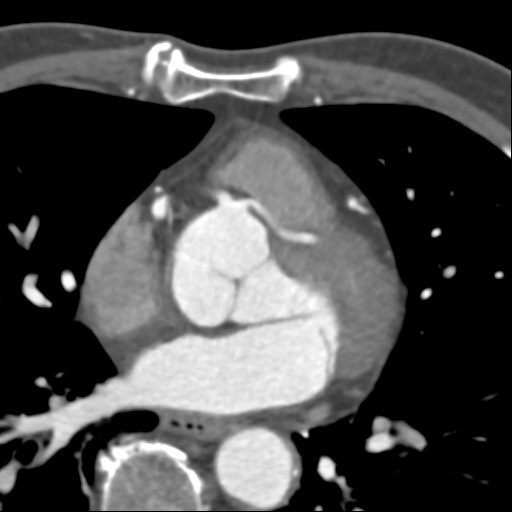 - Relevant catheterization findings:
We performed secondary cardiac catheterization again and it showed 1. CAD (2-V-D) over LAD-P and RCA-D, 2. Abnormal origin of LCA near the orifice of RCA, 3.No LCX. After rechecking the lesion over RCA-D, we deployed DES ONYX 5.0 x22mm to RCA-D, DES ONYX 3.0 x15mmto LAD-P. Under the stable condition, he discharged 2 days later.
|
|
|
[Interventional Management]
- Procedural step:
On 10/19, we had put 6 Fr Pigtail Boston firstly for cardiac structure which no MR or VSD. We used 6 Fr JR4.0 Boston for RCA which showed type B lesion RCA-D with thrombus present. So, we used Tirofiban (12.5 mg/ 50 ml) 13 ml iv bolus for thrombolysis. During the procedure, sustain VT happened and restored after DC shock 200 J. We used 6 Fr JL3.5 Boston but no obvious LCA flow. We tried to change 6 Fr JL4.5 Boston but still failed to find the LCA. We decided to keep thrombolysis first. We would arrange secondary coronary angiogram after 4 days later. We arrange Coronary CTA for the complete evaluation of coronary artery.
On 10/23, we decided guiding with 7Fr SCR4.0 Medtronic and ASAHI SION wire for PCI of RCA. After coronary angiogram, a regressive thrombus over RCA-D was found. We used Vascular GuideLiner V3, 6 Fr for better guiding support. We dilated the RCA-D with NC Emerge 5.0x15 mm to 12 ATM and then deployed DES ONYX 5.0x22 mm up to 14 ATM. After stenting, we used NC Emerge 5.0 x 15 mm, 18 ATM for post-dilatation. When we finished RCA stenting and made the final RCA angiogram showed LCA flow due to some contrast leakage when SCR4.0 with minimal dislocation from RCA. Then we rotated 7 Fr SCR4 Medtronic slowly under the SION wire in RCA support. We successfully engaged into LCA with SCR4 and found the type B lesion over LAD-P. We dilated the stenosis with NC SAPPHIRE II 3.0x12 mm, 12 ATM and then deployed DES ONYX 3.0x15 mm up to 18 ATM. - Case Summary:
About 80% of coronary anomalies are considered benign but it is the second most common causes of exercise related sudden cardiac deaths. In older patient without proximal vessel narrowing, a conservative approach may be reasonable. We still should keep in mind for the diagnosis and risk who had symptoms of ischemia. The technique need to engaging the anomalous origin of coronary artery was dependent to the anatomical relationship by operator individually.
|
|