Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_035
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| STEMI with Coexisted Multiple CTO | |
| Jung-Chi Hsu1, Tung-Lin Tsui2 | |
| National Taiwan University Hospital Jinshan Branch, Taiwan1, Camillian Saint Mary's Hospital Luodong, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mrs. Lo
-Relevant clinical history and physical exam:
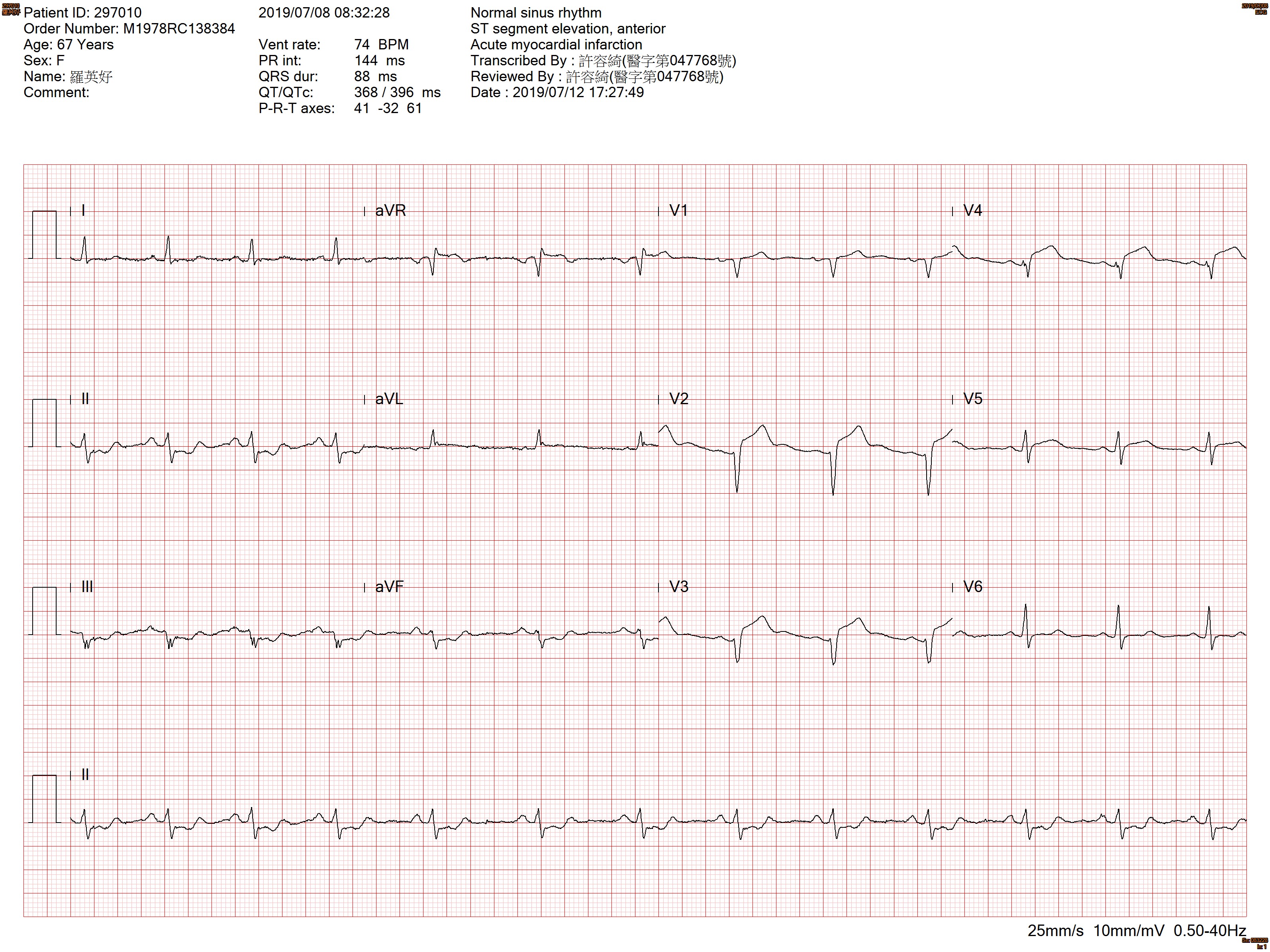
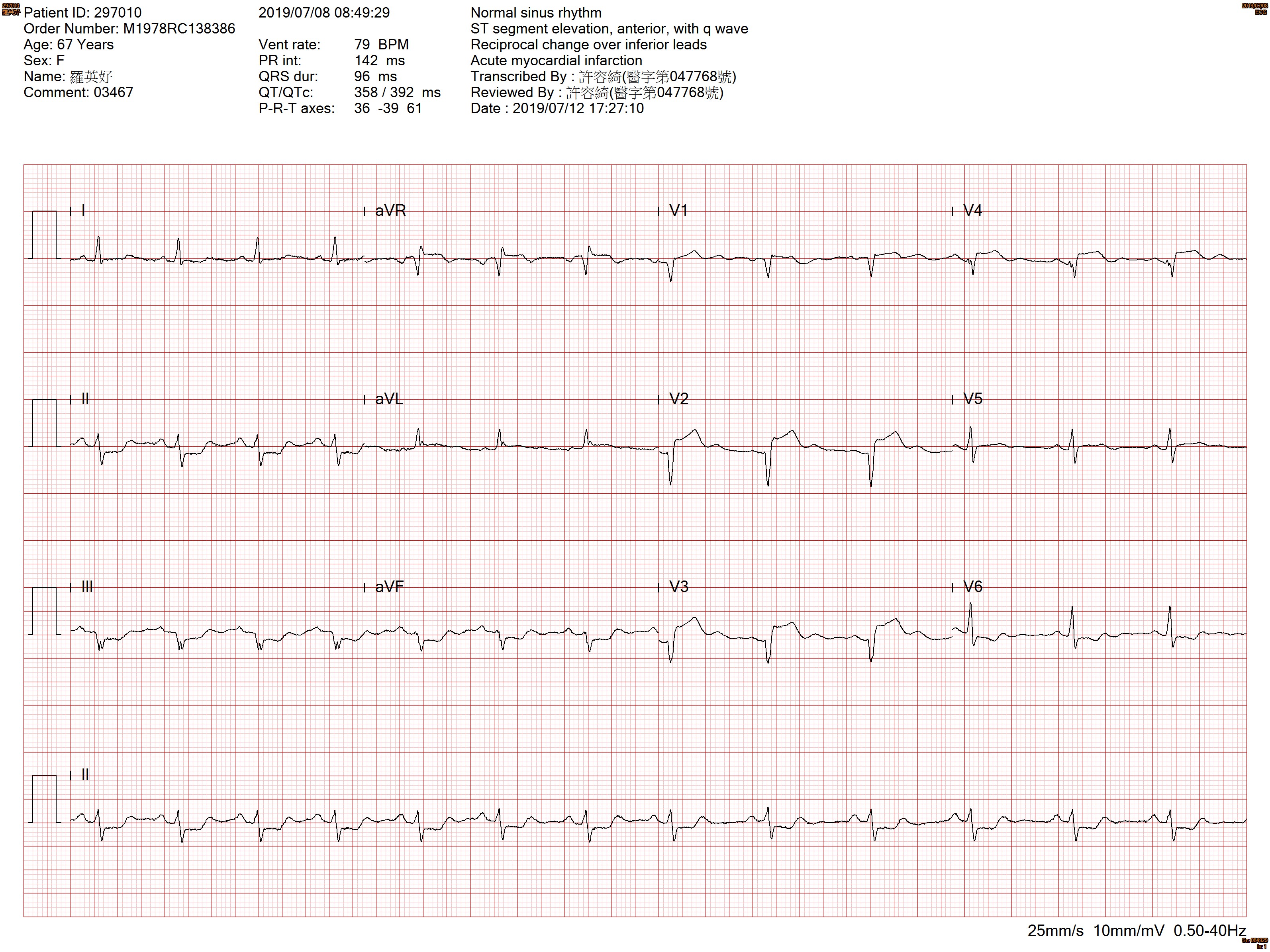
The 67-year-old woman with hyperlipidemia, presented to ER with chest tightness for two days, with bilateral arm numbness.At ER, vital signs, T=36.7; BP=120/77; HR=76ECG showed anterior STEMISTEMI team was initiated.
-Relevant test results prior to catheterization:
ECG showed anterior STEMI with reciprocal change.Dynamic ST more and more elevation was noted.CXR showed mild lung congestion.
   - Relevant catheterization findings:
Coronary Angiogram:
LM: patent LAD: Proximal 100% occlusion, the culprit lesion of STEMI LCX: Aneurysmal change with some floating thrombus over middle LCX, with critical stenosis RCA: proximal to middle total occlusion consider chronic total occlusion, distal retrograde double CTO |
|
|
[Interventional Management]
- Procedural step:
# First attempt: We engaged LCA with EBU GC, wiring to mid LAD but cannot pass. Thrombosuction with Eliminate aspiration catheter and no thrombus. The angiography showed mid LAD CTO. POBA to proximal LAD. With balloon support or buddy wire, the Runthrough Floppy, and Sion wire failed to cross. We changed to CTO wire conquest pro wire. The wire was wiring to small branch with small balloon, false lumen with intramural and epicardial hematoma was noted. After puncture, the distal LAD route appeared and Sion black wire finally went into true lumen. After 2.5mm balloon dilatation from mid to proximal LAD, mid LAD re-occluded. After POBA, deployed 2.5x38, 2.5x38 and 3.0x14 DES to LAD. Post-dilatation over stent and junction with 3.0 NC balloon. The final angiography is TIMI 3 flow. Collaterals to RCA from LAD were noted.# Second attempt: Cardiogenic shock persisted after three days. We performed second look, IABP setup, and revascularized the LCX. With EBU GC and Sion black and Floppy wire to distal LCX and OM. Predilated with small 2.0 balloon to avoid distal embolization and deployed 3.5x18 DES to LCX, and POBA to distal LCX with 2.0 balloon due to size discrepancy. # Third attempt: One month later, tried RCA CTO. Engage RCA with 6Fr AL 1.0 GC, tried XTA, XTR, Sion blue with Finecross, Fielder FC with Caravel, via antegrade. UB3, GAYA2, Sion blue, and conquest pro with Caravel MC via retrograde. Change to AL1.0, SAL 1.5, SCR for support. Rendezvous technique failed. We closed procedure.
- Case Summary:
It is challenging for STEMI patients with proximal LAD total occlusion superimposed on multiple CTO. Mechanical circulation support and CABG should be considered before intervention based on patient's condition and choice. Open the CTO lesion for the culprit vessel is important to preserve the coronary flow, save the heart function, and establish collateral circulation. Complete revascularization with staged PCI for nonculprit CTO will bring the best outcome.
|
|