Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_032
| CORONARY - Drug-Eluting Balloons | |
| In-Stent Chronic Total Occlusion IVUS Guided Treatment with Drug Coated Balloon Eluting Sirolimus and a New DES | |
| Irene Bossi1 | |
| Niguarda Hospital, Italy1, | |
|
[Clinical Information]
- Patient initials or identifier number:
case3 Niguarda
-Relevant clinical history and physical exam:
Female 63 years oldTabagism, hypertension; dyslipidemiaJun 2018 Chronic total occlusion anterograde recanalization of RCA with 2 everolimus eluting stent (Synergy 2.5/48 e Xience 3/38) for angina with normal left ventricle ejection fraction. Sep 2019 Recurrent angina. In-stent total occlusion.
-Relevant test results prior to catheterization:
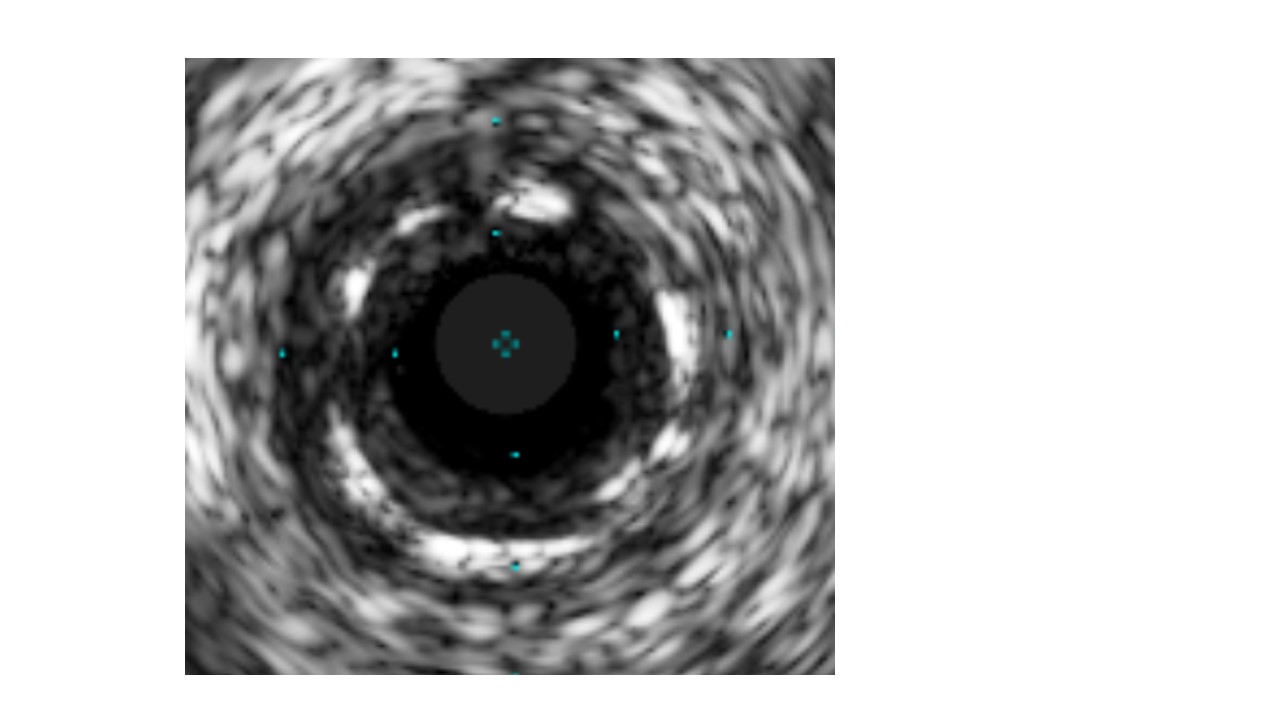
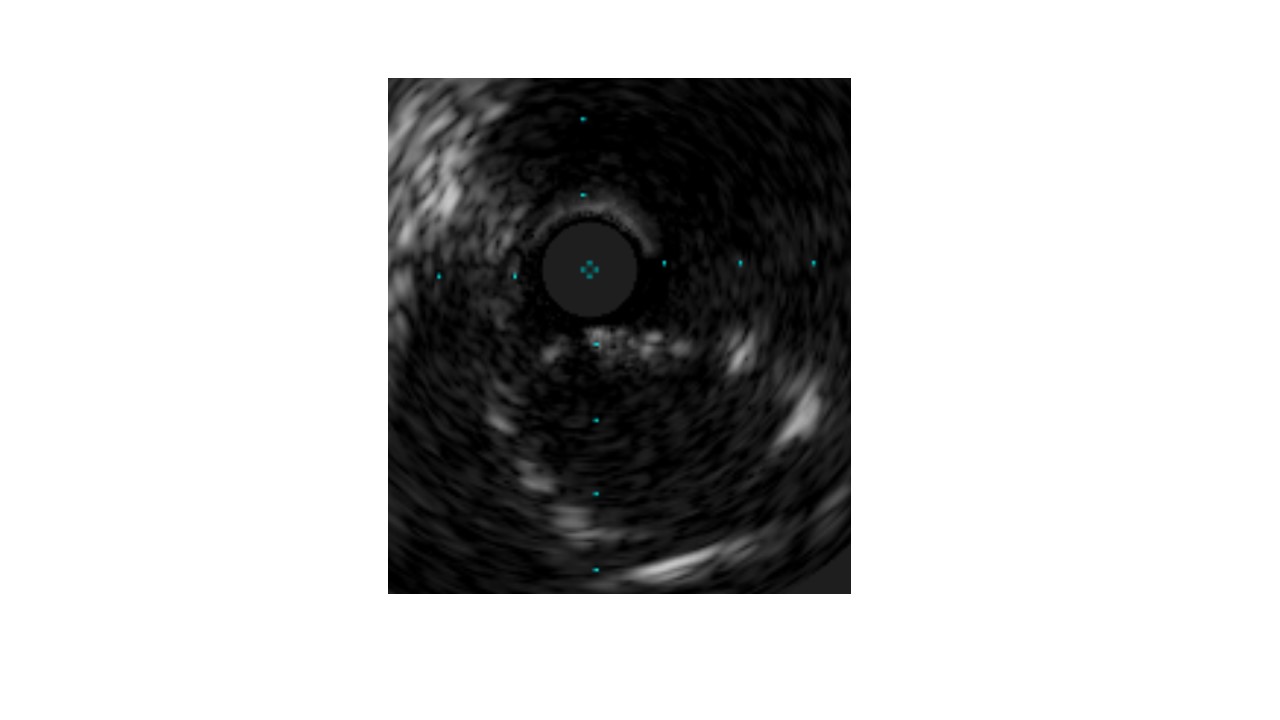
At IVUS the previous implanted stent was undersized with in-stent proliferation at mid RCA an at the ostium the protruding struts were non coaxially cannulated. Reference vessel diameter at mid RCA3.0-3.5, at proximal RCA 4.0-
  - Relevant catheterization findings:
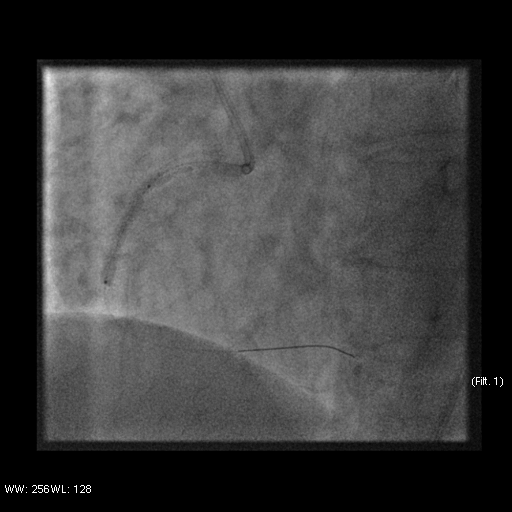
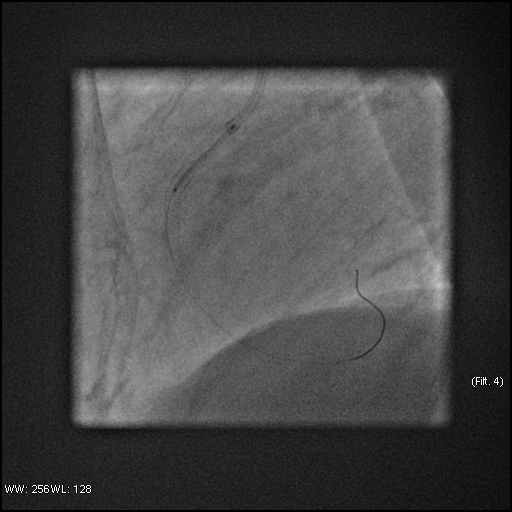
The restenotic lesion was dilated with balloon (Tazuna 2.0/15, Icazuchi 2.5/15). The lesion was then prepared with scoring balloon (Angiosculpt 3.0/15 m) and Non-compliant balloon 3.5/15 mm at 30ATM. After achieving an acceptable angiograpic result, sirolimus was eluted within stents in the mid RCA with 2 drug coated balloon (Magic Touch 3.5/30 mm and 4.0/15 mm) at 10 ATM for 60 seconds. A with a new DES (Tansei Ultimaster 4.0/21 mm) was implanted at the ostium.
  |
|
|
[Interventional Management]
- Procedural step:
RCA restenotic occlusion was crossed with a polymeric wire (Fileder XT) and the support of a microcatheter (Supercross FT) and controlaterale injection. The wire was exchanged with a Sion Blue. The restenotic lesion was dilated with balloon (Tazuna 2.0/15, Icazuchi 2.5/15). IVUS evaluation: reference vessel diameter at mid RCA 3.0-3.5, at proximal RCA 4.0-
- Case Summary:
Historically, ISR represents the first clinical application of drug-coated balloons. The main advantage of DCB is that no new stent scaffold is needed within previously implanted stent. This case represents an example of real-world experience of repeat angioplasty or chronic total occlusion within previously implanted DES. Intracoronary imaging allows for a better understanding of the ISR mechanism, and helps to guide the procedure with a hybrid approach including drug coated balloons and new stent when needed.
|
|