Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_029
| CORONARY - Complications | |
| Aortic Cusp Dissection During Coronary Intervention: A Conservative Approach to a Rare Complication | |
| Khai Chih Teh1, Azhari Rosman1 | |
| National Heart Institute, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
410164
-Relevant clinical history and physical exam:
A 53-year-old gentleman with underlying bronchial asthma, stage II chronic kidney disease and gouty arthritis was referred from a primary care centre for coronary angiogram following a recent inferior myocardial infarction which he was thrombolysed with IV Streptokinase. He had exertional chest pain and reduced effort tolerance NYHA class II. His BP was 138/79, HR 78 bpm with no significant physical findings. He was planned for an elective coronary angiogram and angioplasty.
-Relevant test results prior to catheterization:
ECG: Q waves in leads III, aVF; T inversion in V5 and V6
Echocardiogram: EF 38%, multiple regional wall motion abnormalities with severely hypokinetic apex; mild mitral and tricuspid regurgitation Blood investigations: creatinine 130umol/L (eGFR 53), LDL 1.2mmol/L, HbA1C 5.7%; Troponin T 43 pg/ml 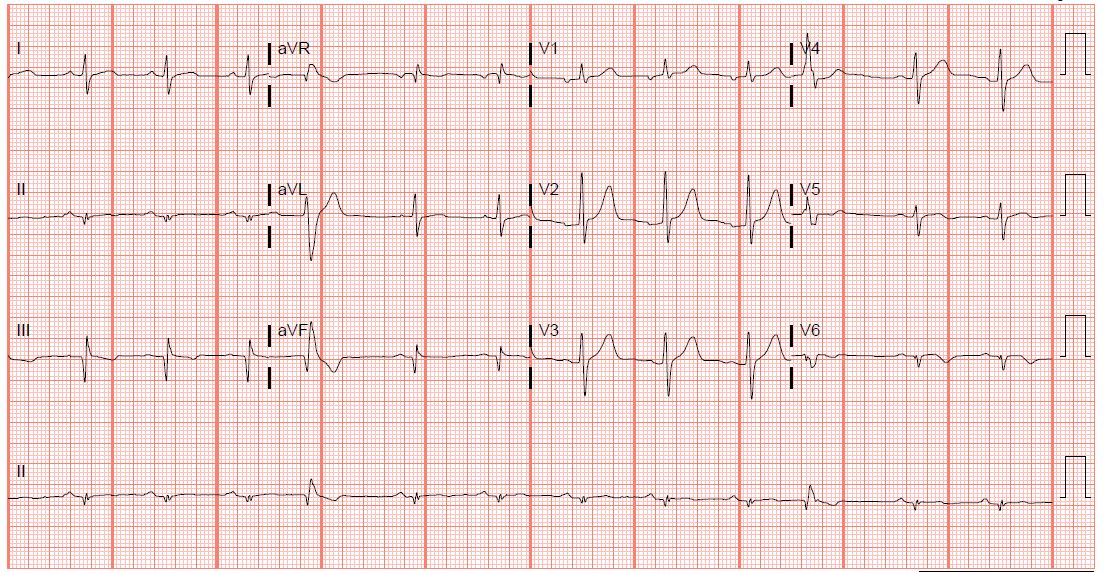 - Relevant catheterization findings:
Coronary angiogram on 18/9/2019
LMS: short, normal LAD: mild disease in mid LAD LCx: Dominant vessel; Chronic Total Occlusion of large OM, retrograde filling PL branchRCA: Small vessel, severe proximal disease We decided for PCI to CTO OM. While attempting to engage guiding catheter EBU 3.5, noted there was contrast staining and retention in the Left Coronary Cusp disseminating around LMS, proximal LAD and LCx which outlined the proximal vessels. |
|
|
[Interventional Management]
- Procedural step:
Procedure was abandoned in view of risk of further dissection and bleeding. Urgent ECHO bedside was performed; no pericardial effusion or aortic regurgitation was noted. Urgent Multislice CT was performed to assess location and degree of dissection. Patient developed ST elevation in precordial leads which resolved on IVI GTN and bedrest. MSCT demonstrated no obvious flap or compromise of coronary vessels indicating spontaneous resolution of the dissection. Patient was discharged and readmitted in 4 weeks for a repeat coronary angioplasty.
Repeat coronary angioplasty was performed on 30/10/2019 showing no residual contrast staining and similar coronary artery findings. Left system was engage with EBU 3.5 and CTO OM was crossed with CROSS-IT 200 wire and FINECROSS microcatheter. Guiding wire was changed to RUNTHROUGH FLOPPY soft wire however during removal of the microcatheter, guiding wire was dislodged from distal OM. Successful re-wiring across the lesion was done with soft wire using a 2.0 mm balloon for support. Sequential pre-dilatation with the existing 2.0 balloon followed by a 2.5 scoring balloon restored flow down the OM. The lesion was stented with a 3.0 x 18mm stent which was upsized to 3.25 proximally with post-dilatation using a 3.25 x 8mm NC balloon. Final results showed TIMI III flow with mild residual disease distal to the stent which was accepted. Stent: XIENCE ALPINE 3.0 x 18mmPost dilatation: NC TREK 3.25 x 8mm at 12 atm - Case Summary:
Patient recovered uneventfully was discharged well with DAPT as well as Sacubitril/ Valsartan for Heart Failure with Reduced Ejection Fraction (HFrEF).
This case illustrates Coronary Cusp Dissection which is a rare, potentially fatal complication during coronary intervention. The etiology is likely trauma to the coronary cusp during manipulation of guiding tip during attempting engagement. Our case was managed conservatively in view of risks of further complications as well as relative hemodynamic stability. Good outcome was achieved from conservative management and PCI was successful on a later date. The emphasis is for cautious and gentle manipulation of all devices during coronary intervention. |
|