Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_028
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| When Imaging Presents IgG4-Related Periarteritis | |
| Jinlong Zhang1 | |
| The Second Affiliated Hospital of Zhejiang University School of Medicine, China1, | |
|
[Clinical Information]
- Patient initials or identifier number:
IHK
-Relevant clinical history and physical exam:
A 70year-old male presented with exertional chest pain to cardiology clinic. The coronary CT angiogram (CTA) performed 8 days ago when he had admitted via emergency departments due to dizziness. He has hypertension for 13 years and family history of coronary artery disease (CAD).
-Relevant test results prior to catheterization:
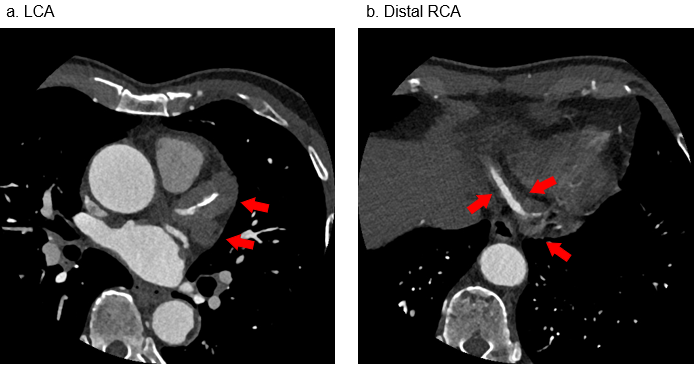
The CT showed multifocal marked wall thickening or well-defined perivascular low attenuation along the coronary artery and over 50% stenosis just proximal to the aneurysm on proximal left anterior descending artery (LAD) diffuse and marked adventitial thickening and enhancement of all coronary arteries, as well as the aortic root and ascending and descending thoracic aorta.
 - Relevant catheterization findings:
With a significantly abnormal IgG4 level (>3x upper limit of normal) and CT, CAG,IVUS finding, a diagnosis of IgG4-related vasculitis was established.
|
|
|
[Interventional Management]
- Procedural step:
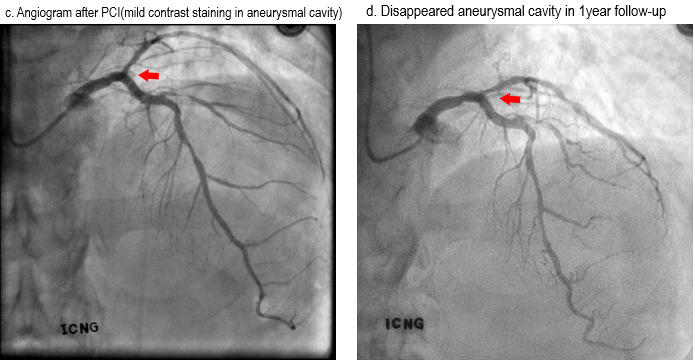
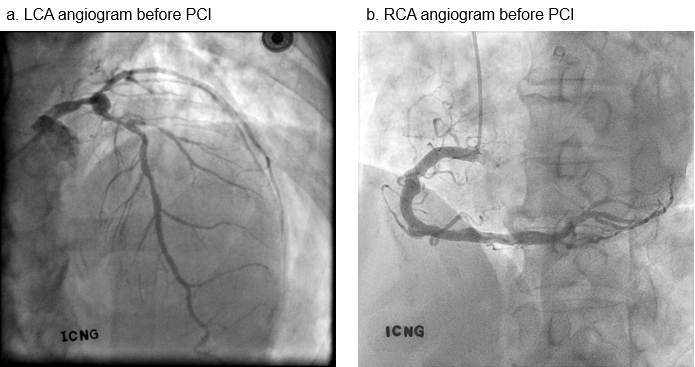
In order to further evaluate his coronary artery disease and the possibility of vasculitis, coronary angiography (CAG) and intravascular ultrasound (IVUS) were performed. Large aneurysmal change in proximal LAD and diffuse stenosis in proximal to mid LAD; diffuse up to 50% stenosis in proximal circumflex artery (LCx); large vessel caliber and uneven luminal contour in proximal to distal right coronary artery (RCA) were observed through CAG. IVUS showed an eccentric calcified plaque minimum lumen diameter < 2mm in LAD. LAD fraction flow reserve was 0.73 with a dramatic step-up through proximal LAD. A drug eluting stent(3.0x28mm) and a graft stent(3.5x19mm) were implanted.
  - Case Summary:
The IgG4-related periarteritis have various imaging finds including aneurysm, stenosis, perivascular thickening, dissection. Moreover, Glucocorticoid therapy and specific therapy should be considered to organ failure.
|
|