Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_015
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Ostial Left Anterior Descending Artery Stenosis, A Left Main Coronary Artery Disease: Where to Put the Stent? | |
| Nazim Megherbi1, Mohamed Abed Bouraghda, Mohamed Bouafia4, Mohamed Tahar Chafik Bouafia | |
| King AbdulAziz Specialist Hospital, Saudi Arabia1, CHU Frantz Fanon, Algeria4, | |
|
[Clinical Information]
- Patient initials or identifier number:
A.M.
-Relevant clinical history and physical exam:
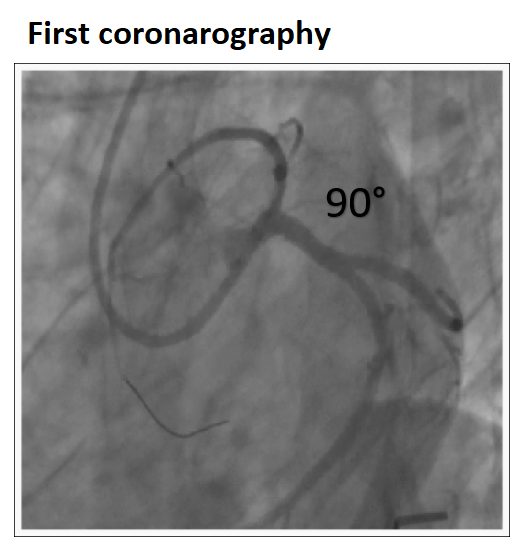
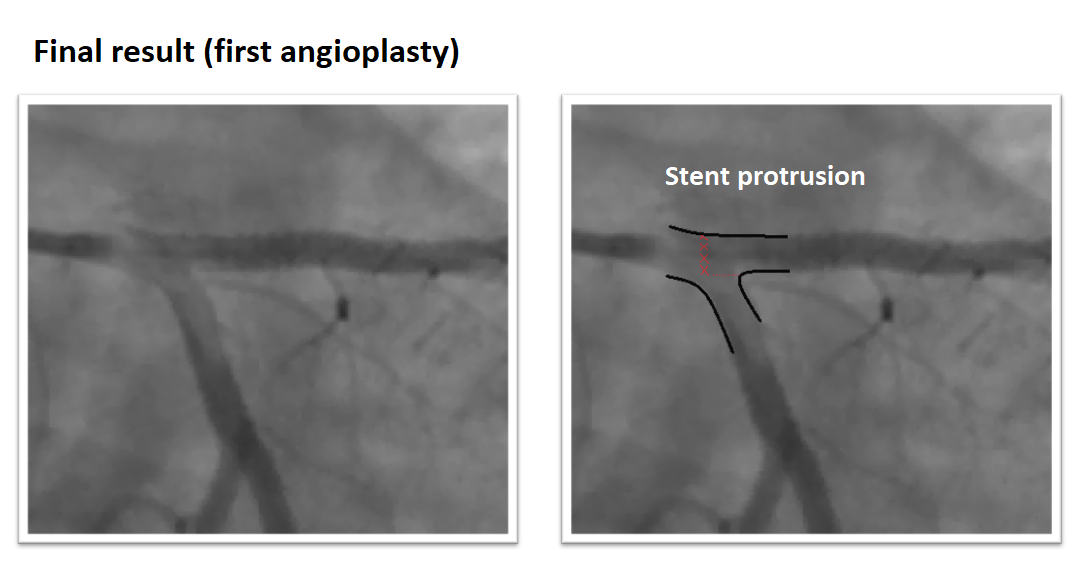
Our patient is a 46-year-old diabetic woman admitted for high-risk non ST elevation myocardial infarction (NSTEMI) with severe chest pain. She was hemodynamically stable. Two years ago, she was hospitalized for high-risk NSTEMI with tight stenosis of the ostial left anterior descending artery (LAD) at the coronarography. The patient had a just ostial angiolasty technique with incorrect placement and a prominent protrusion of the stent in the circumflex lumen.
  -Relevant test results prior to catheterization:
The very high risque NSTEMI was related to a transient ST elevation in inferior leads, troponin elevation was at 24 times normal limits. Echocardiography showed hypokinesia in inferior wall with ejection fraction around 53%.
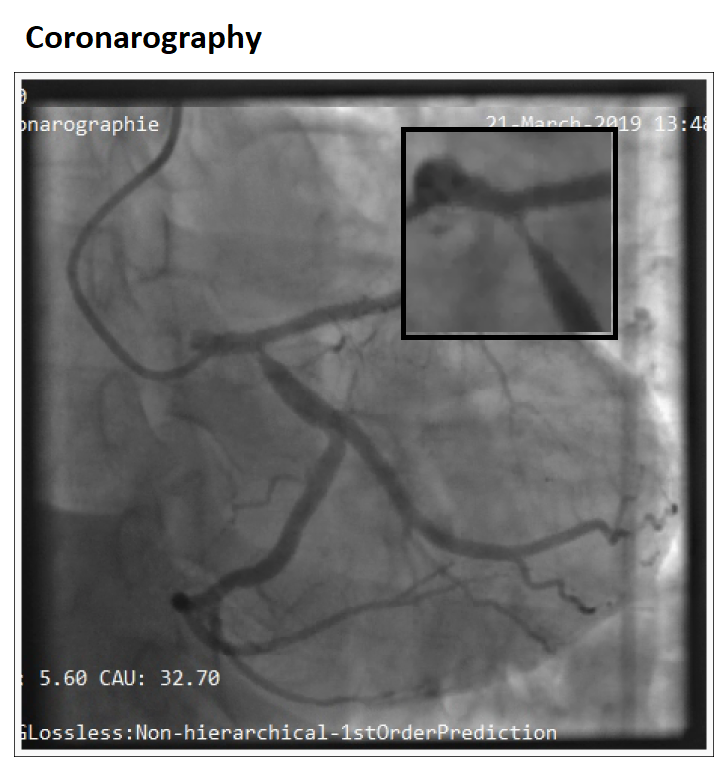
- Relevant catheterization findings:
The coronarography showed a very tight stenosis of the ostial circumflex adjacent to the stent protrusion, the lesion was thrombotic. There was no intra stent restenosis on the ostial LAD.
 |
|
|
[Interventional Management]
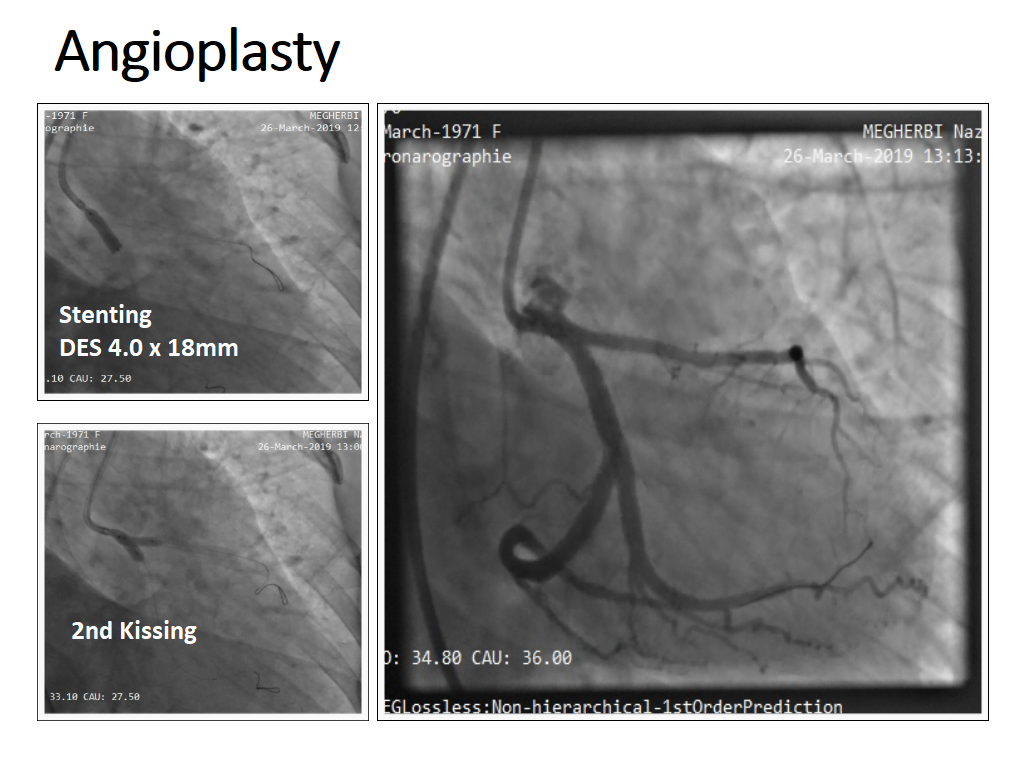
- Procedural step:
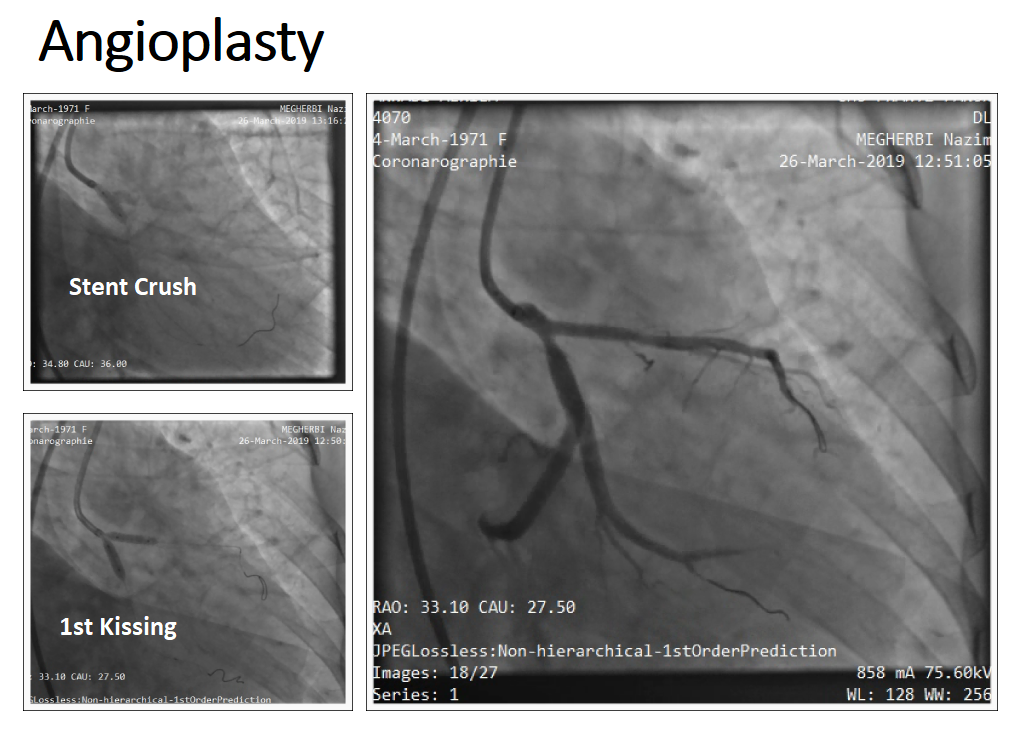
The stent on the LAD was free of intrastent stenosis with prominent protrusion on the left main (LM). The diameter of the circumflex (CX) was 4 mm. The ostial CX was involved (MEDINA 0.1.0). For all these arguments, we considered a DK-Crush technique given the stent already deployed on the LAD as a side-branch stent. We crushed the protruded part of the stent on the LAD with a 4.0x 12mm NC balloon. After wire exchange, we performed a kissing balloon with the 4.0 x 12mm NC balloon and a 3.0 x 12mm NC balloon. We deployed the second DES 4.0 x 18mm in the left main to the circumflex. We performed the second kissing balloon and a final POT using a 5.0x 8mm NC balloon with a satisfying final angiographic result.
  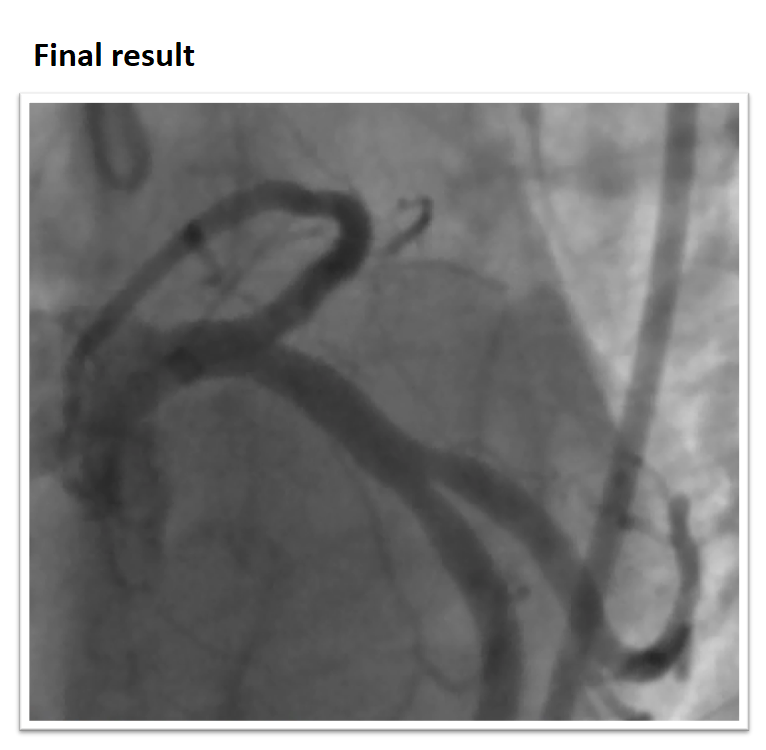 - Case Summary:
Ostial stenosis of the anterior descending anterior artery is considered complex angioplasty. These are left main bifurcation lesions (Medina class 0.1.0). The choice between just ostial LAD angioplasty or angioplasty extended to the left main obeyed to several criteria where the most important is to ensure perfect positioning and plaque coverage if the stent is just proximal. In case of restenosis with stent protrusion, the most appropriate technique is probably DK-Crush bifurcation angioplasty.
|
|