Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_011
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Bifurcational Drug-Eluting Stents: A Good Option for "True" Bifurcations Treatment | |
| Plamen Todorov Penchev1, Farhat Fouladvand2, Sashko Zhezhovski3, Nikolay Dimitrov4 | |
| "Heart and Brain" - Burgas, Bulgaria1, Clinica San Carlo, Italy2, Bulgarian Cardiac Institute, Bulgaria3, University Hospital St. Ekaterina, Bulgaria4, | |
|
[Clinical Information]
- Patient initials or identifier number:
GRG
-Relevant clinical history and physical exam:
A 73-year-old male was hospitalized for dyspnea and chest discomfort at minimal physical exertion. The onset of his symptoms was some weeks earlier. Visiting his GP an unknown by this moment LBBB was registered on the ECG and he was reffered for invasive coronaryangiography. The patient had history of poorly controlled arterial hypertension without regular medication and COPD on inhalatory therapy with rare exacerbations.
-Relevant test results prior to catheterization:
At the admission the patient was stable with normal blood pressure, slightly increased heart frequency ( 100 beats/min) and a faint systolic murmur in themitral region. On ECG we registered sinus rhythm and LBBB. All laboratory testswere in normal ranges except the elevated cholesterol values. On ultrasound we found enlarged left ventricle, decreased EF with apical and lateral hypokinesia and moderate mitral regurgitation. The calculated GRACE score was 125.
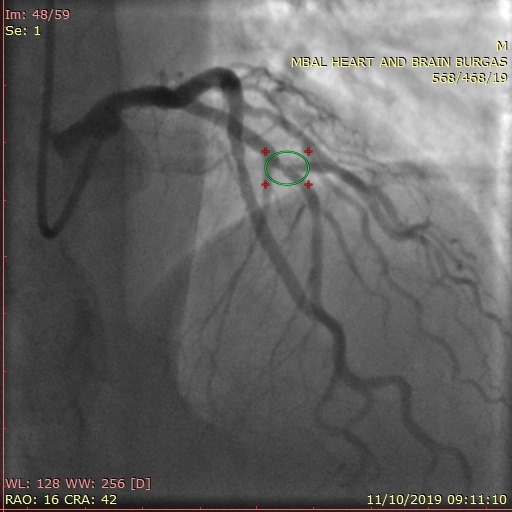
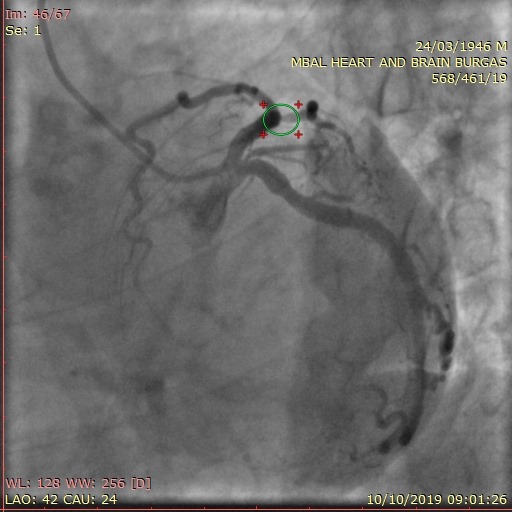
- Relevant catheterization findings:
We used right radial access for the angio. The left angiogram revealed significant stenosis at the bifurcation of LAD and first diagonal branch, that had critical ostial stenosis, another moderate stenosis in the distal part ofLCX and 40% stenosis at the ostium of a large OM.RCA had no significant lesions.- The patient refused anyfurther intervention. Next day after a new conversation and increasing values of troponin in the background he gave aninformed consent for PCI.
  |
|
|
[Interventional Management]
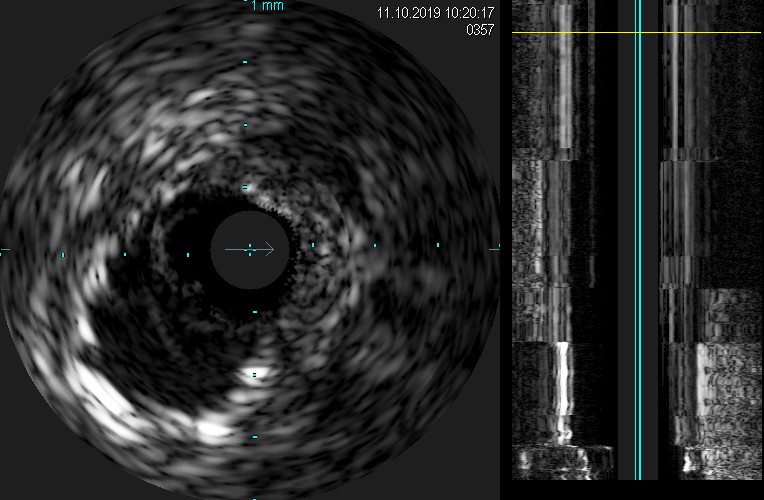
- Procedural step:
The target was the “true” bifurcation (Medina 1,1,1) in LAD and RD 1. Our dilemma was provisional stenting or a two-stent strategy. We decided to use dedicated bifurcational DES. After placing 6 Fr guiding catheter EBU 3.5 we crossed the lesion with two 0,014”guidewires Terumo Runthrough NS in LAD and RD 1. A predilatation of the ostium of RD 1 was done with a 2.0/15 mm Artimes semi-compliant balloon and one bifurcational stent Biomime Branch 3.0-2.5/24 mm was placed towards the diagonal branch. Next we did proximal postdilatationwith 3.5/8mm Apollo NC balloon and after translocating the guidewire from RD 1 into the distal part of LAD inserted another DES Supraflex3.0/36mm, overlapping the proximal part of the first stent. Next angiogram revealed significant plaque shift and thrombosis in the ostium of RD 1. We applied tirofiban and after re-crossing the ostium of the diagonal branch with second guidewire did kissing inflation with two Apollo NC baloons – 3.25/20 mm in LAD and 2.5/15 mm in RD 1 with a good angiographic result. IVUS done revealed good side-branch ostium and suboptimal appostion of the stents in proximal LAD. We did optimization with NC baloon 4.0/10mm and the final angio and IVUS were acceptable. The patient was discharged on the next day ingood clinical condition.
   - Case Summary:
The successful treatment of coronary bifurcations is still a technical challenge. Using dedicated bifurcational DES is a viable option in case of a “true” bifurcation. The proper action sequence and the use of IVUS is mandatory in such cases.
|
|