Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_005
| CORONARY - Stents (bare-metal, drug-eluting) | |
| Keep It Simple Strategy - Left Main Intervention of Patient with Pancreatic Ampullary Carcinoma | |
| Yee Sin Tey1, Yau Piow Ng1, Shaiful Azmi Yahaya1 | |
| National Heart Institute, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
OS
-Relevant clinical history and physical exam:
68 years old gentleman who had dyslipidaemia, hypertension and chronic kidney disease (stage 3A). He was diagnosed to have pancreatic ampullary carcinoma and planned for Whipple Procedure. He was referred to us for pre-operative cardiac assessment. He had been having stable angina (CCS III) for a year. Clinical examination was unremarkable. Dobutamine Stress Echocardiogram showed ST depression at inferolateral leads with hypokinesia at LAD territories during peak exercise.
-Relevant test results prior to catheterization:
Full Blood Count: TWC 4.8x109/L, Hb 11.1 g/dL, PLT 235x109/L Liver Function Test: Albumin 40 g/L, ALP 129 U/L, ALT 23 U/L, T Bilirubin 5 umol/LHbA1c: 5.6%Fasting Lipid Profile: T Chol 2.3 mmol/L, Triglycerides 1.3 mmol/L, LDL 1.0 mmol/L, HDL 0.7 mmol/LRenal Function Test: Urea 4.7 mmol/L, Creatinine 130 umol/L (eGFR 48)Echocardiogram: Left Ventricular Ejection Fraction 58%. No regional wall motion abnormalities. No significant valvular abnormalities.
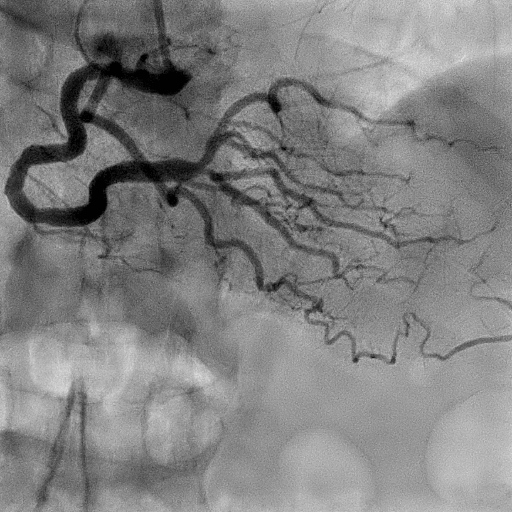
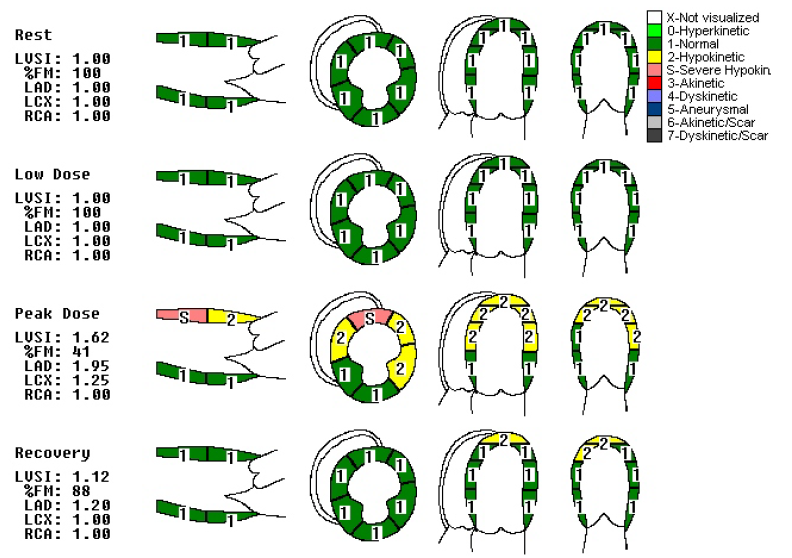 - Relevant catheterization findings:
Left Main: Tight stenosis at distal segment Left Anterior Descending Artery: Tight stenosis from left main to ostium. Ectatic at proximal Left Circumflex: Normal Right Coronary Artery: Moderate stenosis at distal RCA / bifurcation
 |
|
|
[Interventional Management]
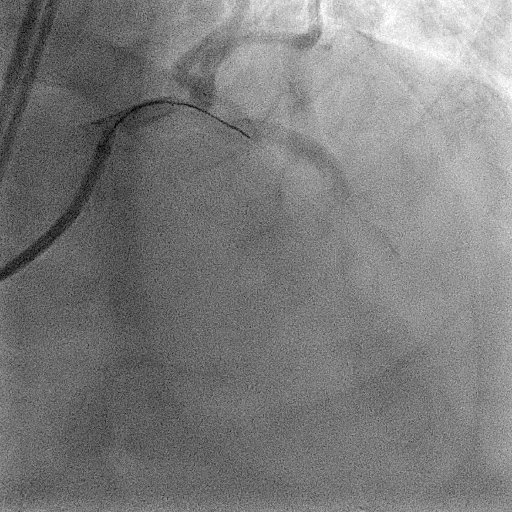
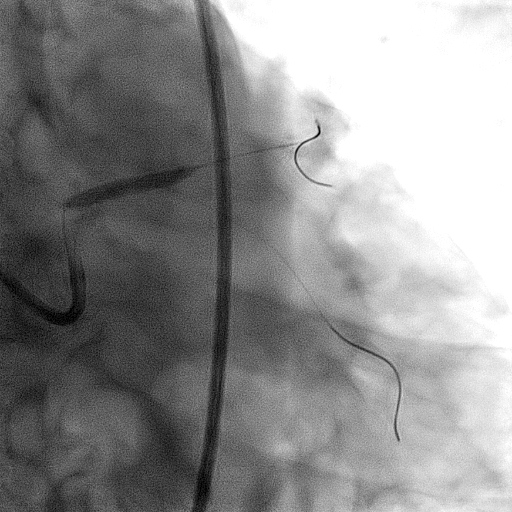
- Procedural step:
Patient had refused coronary artery bypass surgery. Coronary intervention with Intravascular Ultrasound (IVUS) Guidance was planned. Right femoral approach was adopted. Guiding catheter JL 4.0/7 Fr was used with Runthrough floppy wire at LAD and Sion Blue wire at LCX. Distal left main was predilated with Mozec 3.0/20mm balloon at 6 atm to allow advancement of IVUS. IVUS showed heavy plaque burden at distal LM to ostial LAD. Left Main artery size of 5.0mm. Polymer Free Drug Coated Stent Biofreedom 4.0x24mm stent was deployed at mid-LM to proximal LAD. Stent was postdilated with Non-Compliant balooon Emerge 4.0/12mm at 14-22 atm followed by post-dilatation of left main with Non-Compliant Balloon Emerge 5.0/8mm at 14 atm. IVUS showed well apposition of stent.
  - Case Summary:
Early surgical intervention of pancreatic ampullary carcinoma offered better long term outcome. Unfortunately this patient had concurrent critical left main disease warranted coronary intervention before major non-cardiac surgery. Percutaneous approach would be more feasible in this case with polymer free drug coated stent at left main to left anterior descending artery. This offered early recovery with shorter duration of dual antiplatelet therapy.
|
|