Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_002
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Physiologic Lesion Assessment | |
| Do Miracles Happen?: Complete Regression of Coronary Atherosclerosis | |
| Hak Seung Lee1, Mineok Chang2, Bon-Kwon Koo3 | |
| Medical AI, Korea (Republic of)1, Vuno Inc, Korea (Republic of)2, Seoul National University Hospital, Korea (Republic of)3, | |
|
[Clinical Information]
- Patient initials or identifier number:
SJY
-Relevant clinical history and physical exam:
A 44-year-old woman without any cardiovascular risk factors presented with a 2-month history of exertional angina. The patient had no history of hypertension, diabetes mellitus, dyslipidemia, or smoking.
-Relevant test results prior to catheterization:
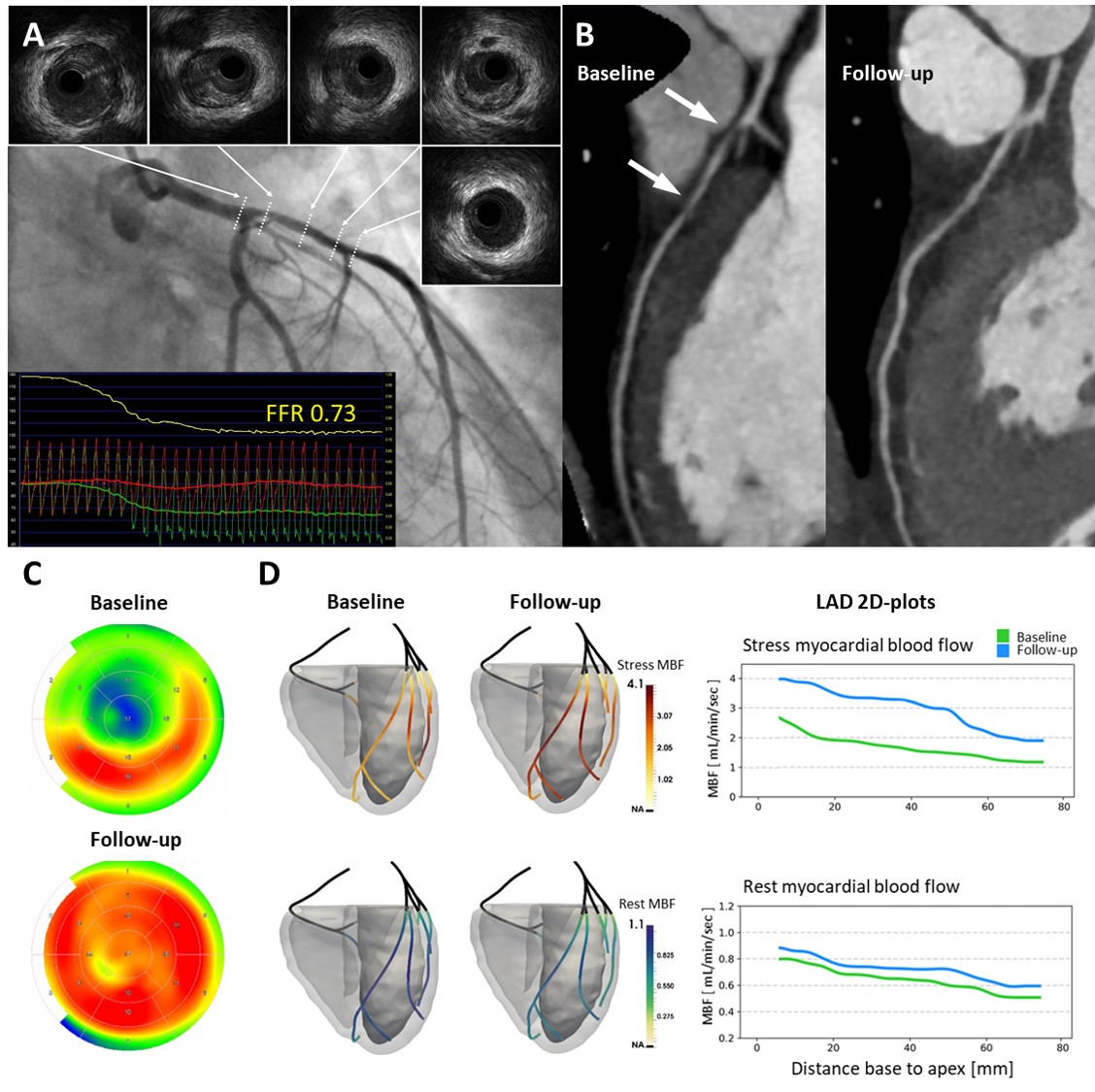
Coronary computed tomographic angiography (CCTA) showed 70% stenosis of the proximal left anterior descending (LAD) artery by non-calcified plaque, and N-13 ammonia positron emission tomography (PET) demonstrated the reversible perfusion defect in the LAD territory (Panels B and C).
- Relevant catheterization findings:
Invasive coronary angiography revealed diffuse intermediate stenosis in the LAD. Fractional flow reserve was 0.73 and the gradual increase of FFR was observed during pull-back pressure tracings under hyperemia (Panel A, yellow line). Intravascular ultrasound revealed diffuse plaque in the left main and LAD with negative remodeling. Minimal lumen area was 3.0 mm2 with plaque burden of 55%.
|
|
|
[Interventional Management]
- Procedural step:
Based on the patient’s preference and lesion characteristics, medical treatment with aspirin, ezetimibe/simvastatin, and diltiazem was initiated and maintained during follow-up. The patient’s symptoms disappeared around 1 year after medical treatment. Three years later, repeat PET showed normal perfusion in the LAD territory with preserved coronary flow reserve (Panel B). Follow-up CCTA showed complete regression of the atherosclerotic plaque at the proximal LAD (Panel C). Image fusion techniques of dynamic PET and CCTA were applied to this patient, and these images showed a 3D display of the coronary physiology along the LAD at baseline and follow-up (Panel D).
 - Case Summary:
Complete plaque regression is a rare but impressive entity, which should be attentively investigated. The present case suggests that medical treatment with careful follow-up can be an option in selected patients with coronary artery disease.
|
|