Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_001
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| Saving a Limb with Intra-Arterial Thrombolysis | |
| Sunanto Ng1 | |
| Universitas Pelita Harapan, Indonesia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
SD.SHLV.845312
-Relevant clinical history and physical exam:
A 53-year-old man complained of sudden pain of his left hand one hour before admission to the emergency department. He could not make any movement of his left hand. His cardiovascular risk factor was smoking, diabetes mellitus and hypertension. The blood pressure was 180/85 mmHg, heart rate of 108 bpm, Oxygen saturation of right hand was 98%; while of the left hand was 73%. The left hand was felt cold, cyanotic and painful with pain scale 9/10. Pulsation of left radial artery was very weak.
 -Relevant test results prior to catheterization:
ECG revealed sinus rhythm with dominant S wave in V1-4 suggesting left ventricle (LV) enlargement. Echocardiography confirmed LV dilatation with LV ejection fraction of 28%; akinetic inferior wall and hypokinesia of other segments. No apparent thrombus was seen. Hemoglobin level was 14.3 g/dL; platelet count 123000 /mL, creatinine level 1.1 mg/dL (estimated glomerular filtration rate 69 mL/min/1.73 m2) and increased D-dimer level (2.2 mg/mL).
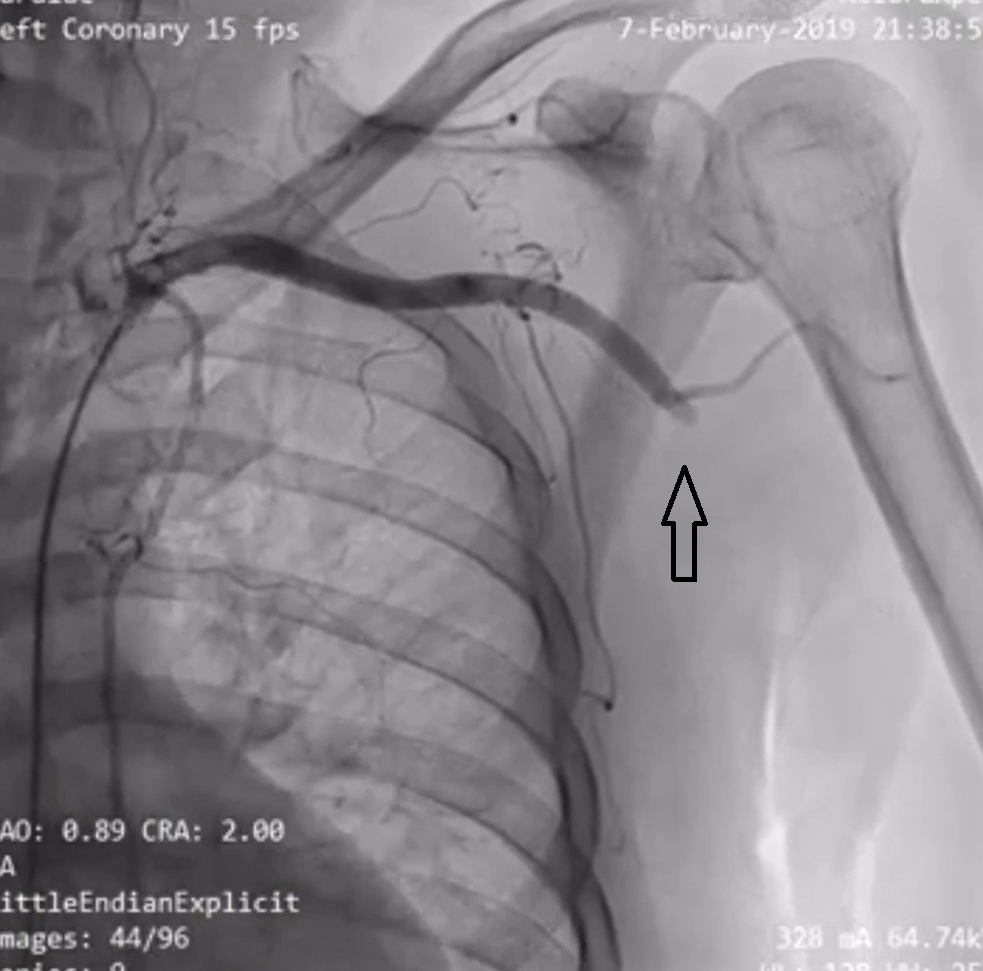
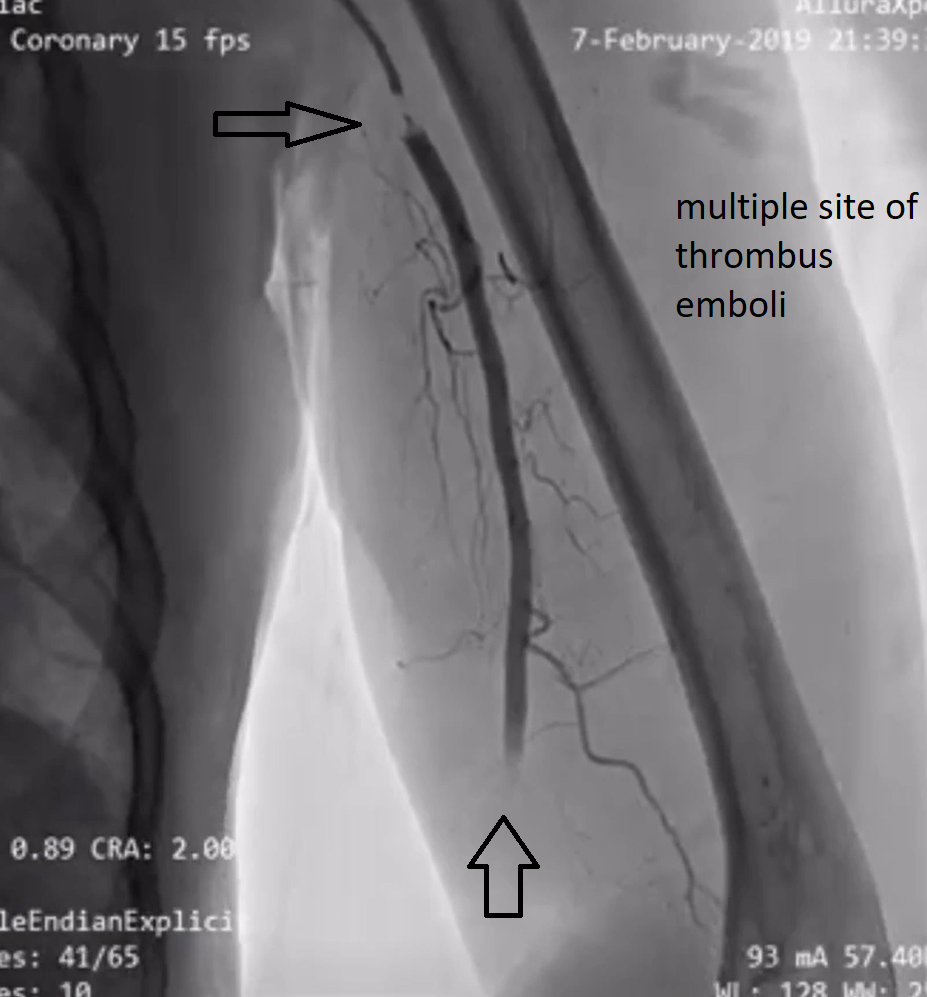
- Relevant catheterization findings:
Patient was urgently sent for angiography of the extremity and concurrently coronary. The access was right femoral artery. Coronary angiography revealed significant lesion of mid left anterior descending artery and proximal of left circumflex artery. Left upper extremity angiography non-occlusive thrombus at the proximal subclavian artery and totally occluded of brachial artery
  |
|
|
[Interventional Management]
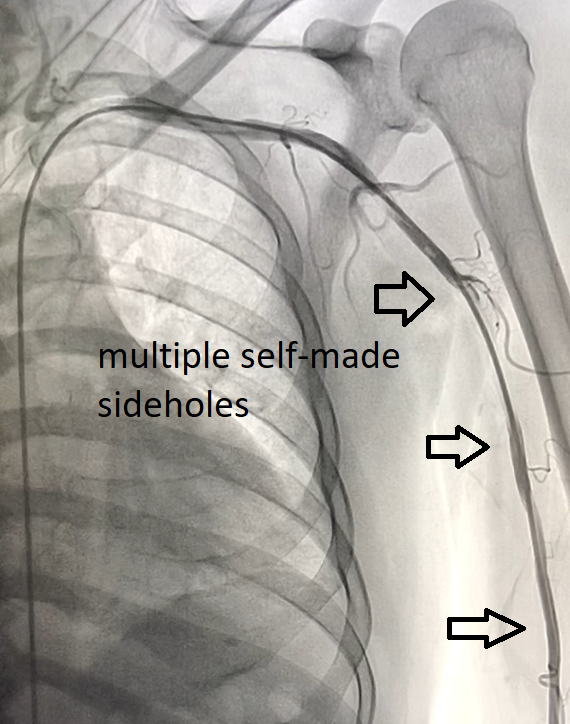
- Procedural step:
Judkin right 3.5/6F catheter was used for intra-arterial thrombolysis. Two sites of side-holes was made; one site was near the tip (distal side-holes) and another site was made 15-20 cm from the tip (proximal side-holes). The configuration of proximal side-hole was to provide entry point of blood flow to the tip catheter so that distal limb can get perfusion. The distal side-holes was to deliver thrombolysis agent to the thrombus. Alteplase was used as the thrombolysis agent. One mg was given bolus through the catheter; continued with infusion dose of 1 mg/hour. Additionally, unfractionated heparin was given intravenously 100 unit/hour.
 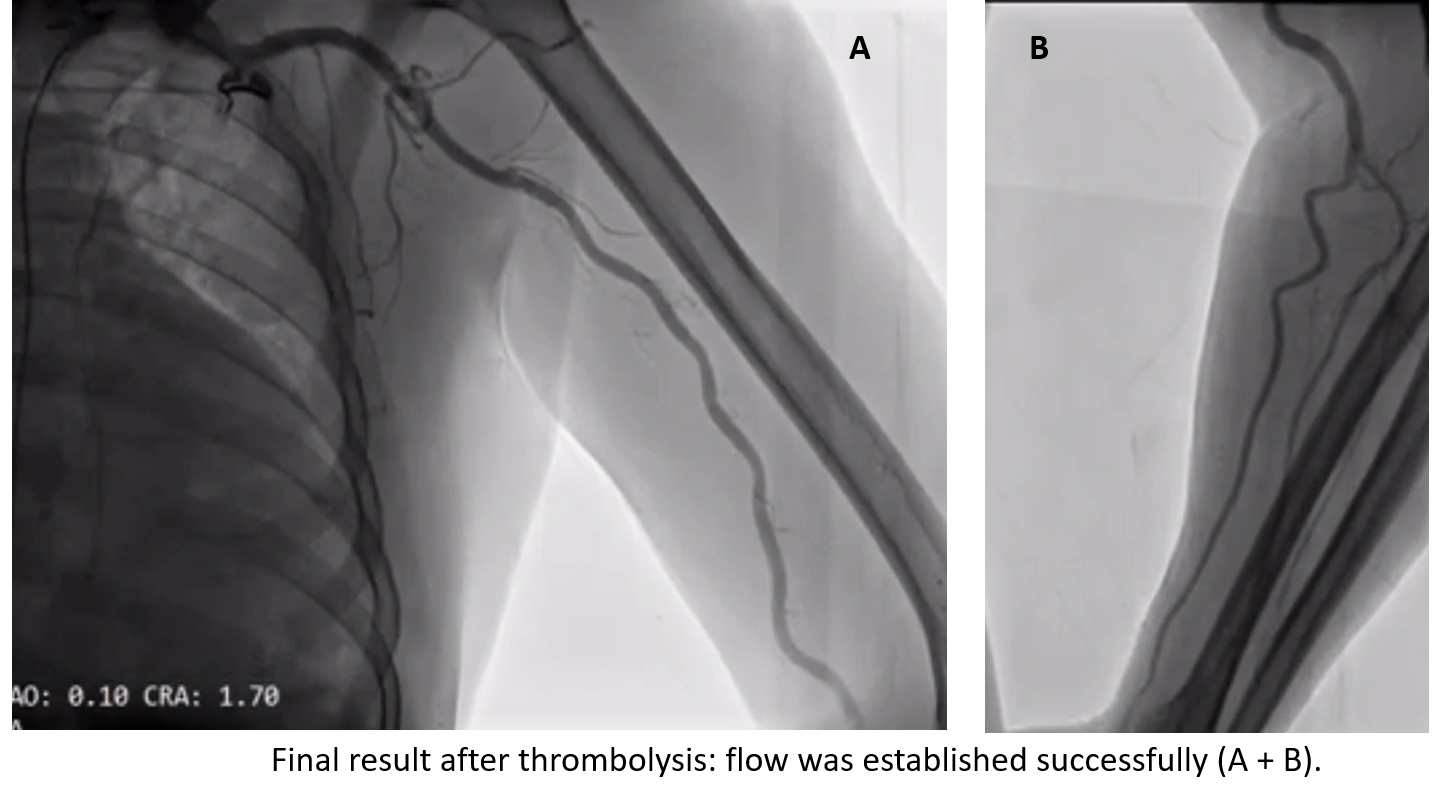  - Case Summary:
In conclusion, intra-arterial catheter-directed thrombolysis is essential method for salvation of acute limb ischemia due to thrombus occlusion. Side-holes for the catheter can be used to provide temporary perfusion route to prevent limb infarction. This method is cheap, safe and easily to be done.
|
|