Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_019
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| A Rare Case of Percutaneous Coronary Intervention in Dextrocardia and ST Elevation Myocardial Infarction | |
| Chong Wei Loong1, Houng Bang Liew2 | |
| KPJ Sabah Specialist Hospital, Malaysia1, Queen Elizabeth II Hospital, Malaysia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
BD
-Relevant clinical history and physical exam:
68-year-old gentleman with history of hypertension and dyslipidaemia presented to a district hospital with sudden onset of resting chest pain. Upon presentation, he was haemodynamically stable. Cardiovascular examination revealed right sided apex beat.
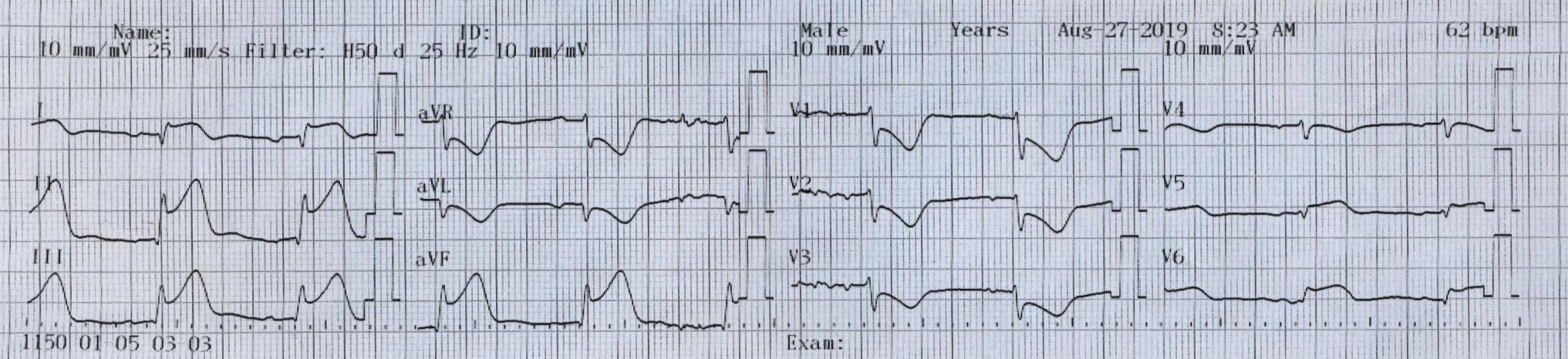
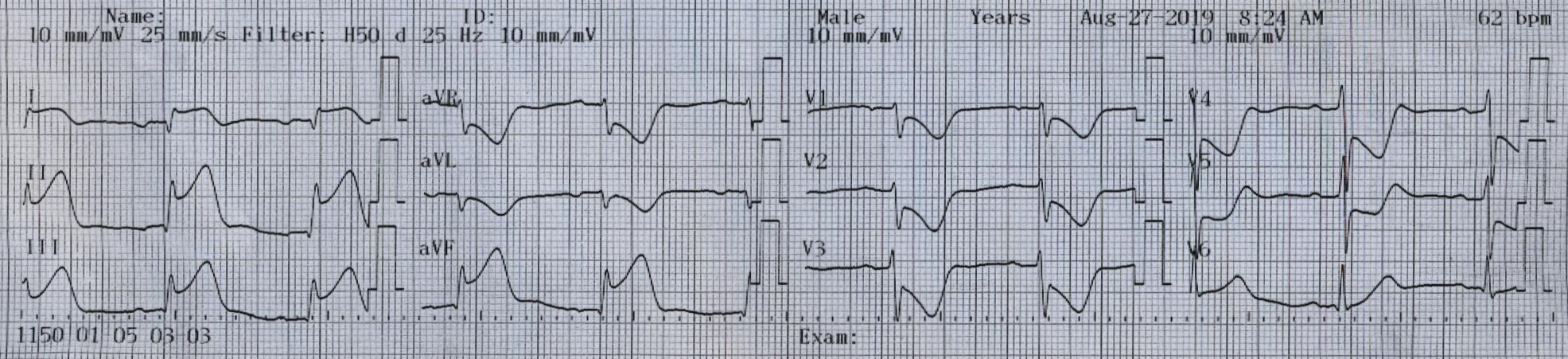
-Relevant test results prior to catheterization:
The 12 leads electrocardiogram showed ST elevations in leads II, III, aVF, V5-V6, ST depressions in leads V1-V3 and low voltages in leads V3-V6. Right sided chest leads showed prominent R waves. Thrombolytic therapy was started. He was referred to our center for rescue angioplasty after failed thrombolytic therapy.
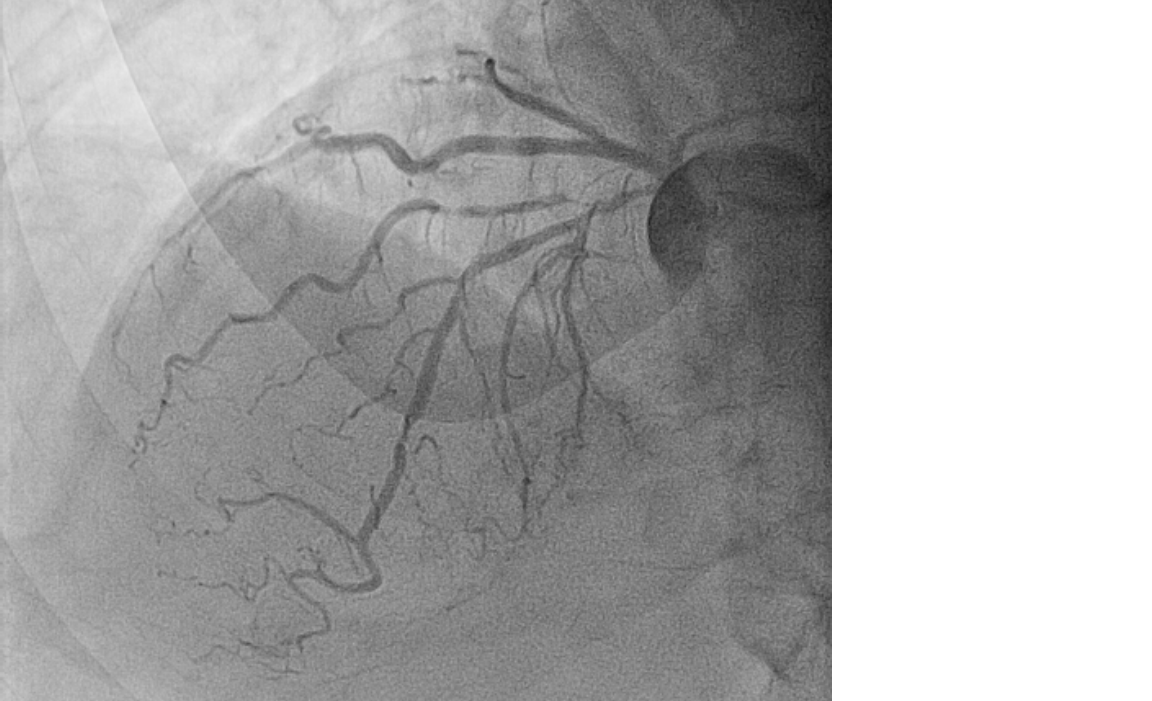
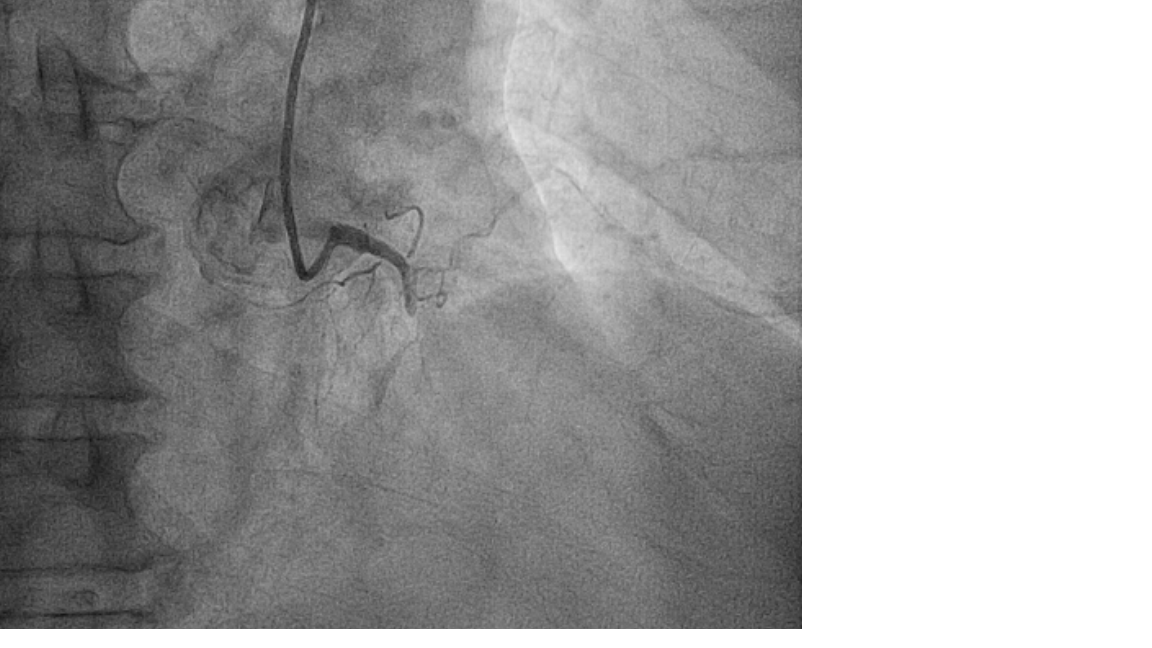
  - Relevant catheterization findings:
The procedure was performed via right radial assess using a 6 French system. The left coronary artery was cannulated with Optitorque catheter (5Fr, Terumo). The left coronary artery was on anatomically right side. Mid left anterior descending artery 80% stenosis. The right coronary artery (RCA) was cannulated with the same Optitorque catheter in anti-clockwise rotation at right anterior oblique view. The RCA was dominant and anatomically on the left side. The proximal RCA was occluded.
  |
|
|
[Interventional Management]
- Procedural step:
We proceed with percutaneous coronary angioplasty to the right coronary artery. The right coronary artery was selectively engaged with a 6Fr Judkin left catheter and the lesion was crossed with the Pilot 50 guidewire (Abbot vascular). Pre-dilatation to the proximal right coronary artery was performed with a Sprinter Legend balloon (2.0x12mm, Metrodnic) and a Biofreedom drug eluting stent (3.5x24mm, Biosensors International Ltd) was deployed at 12 atmosphere pressure. Post-dilatation was carried out using NC TREK balloon (3.5x8mm, Abbot Vascular) at 24 atmosphere pressure. TIMI 3 flow achieved.
   - Case Summary:
We report a rare case of successful percutaneous coronary intervention in a patient with dextrocardia and acute myocardial infarction. We demonstrated that coronary angioplasty in dextrocardia via trans-radial approach can be performed effectively with appropriate technical modifications.
|
|