Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_011
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| Intentional Detour Creation by ADR in Calcified CTO Impassable to Devices after Successful Guidewire Passage | |
| Masato Ishikawa1, Atsunori Okamura2, Hiroyuki Nagai3, Kota Tanaka1, Satoshi Suzuki1, Akinori Sumiyoshi4, Mutsumi Iwamoto1, Kenshi Fujii1 | |
| Sakurabashi Watanabe Hospital, Japan1, Sakurabashi Watanabe Advanced Healthcare Hospital, Japan2, Saint Joseph's Translational Research Institute, USA3, Sakurabashi Watanabe Advanced Health care Hospital, Japan4, | |
|
[Clinical Information]
- Patient initials or identifier number:
H.S
-Relevant clinical history and physical exam:
A 78 years old female was admitted to previous hospital due to heart failure. She had dyslipidemia, paroxysmal atrial fibrilation, and the past gustolic ulcer. Coronary angiography revealed the significant stenosis with severe calcification in the mid-LAD during hospitalization. 1st PCI was tried at previous institution, any balloon catheter could not passed through the lesion because of the severe calcification. 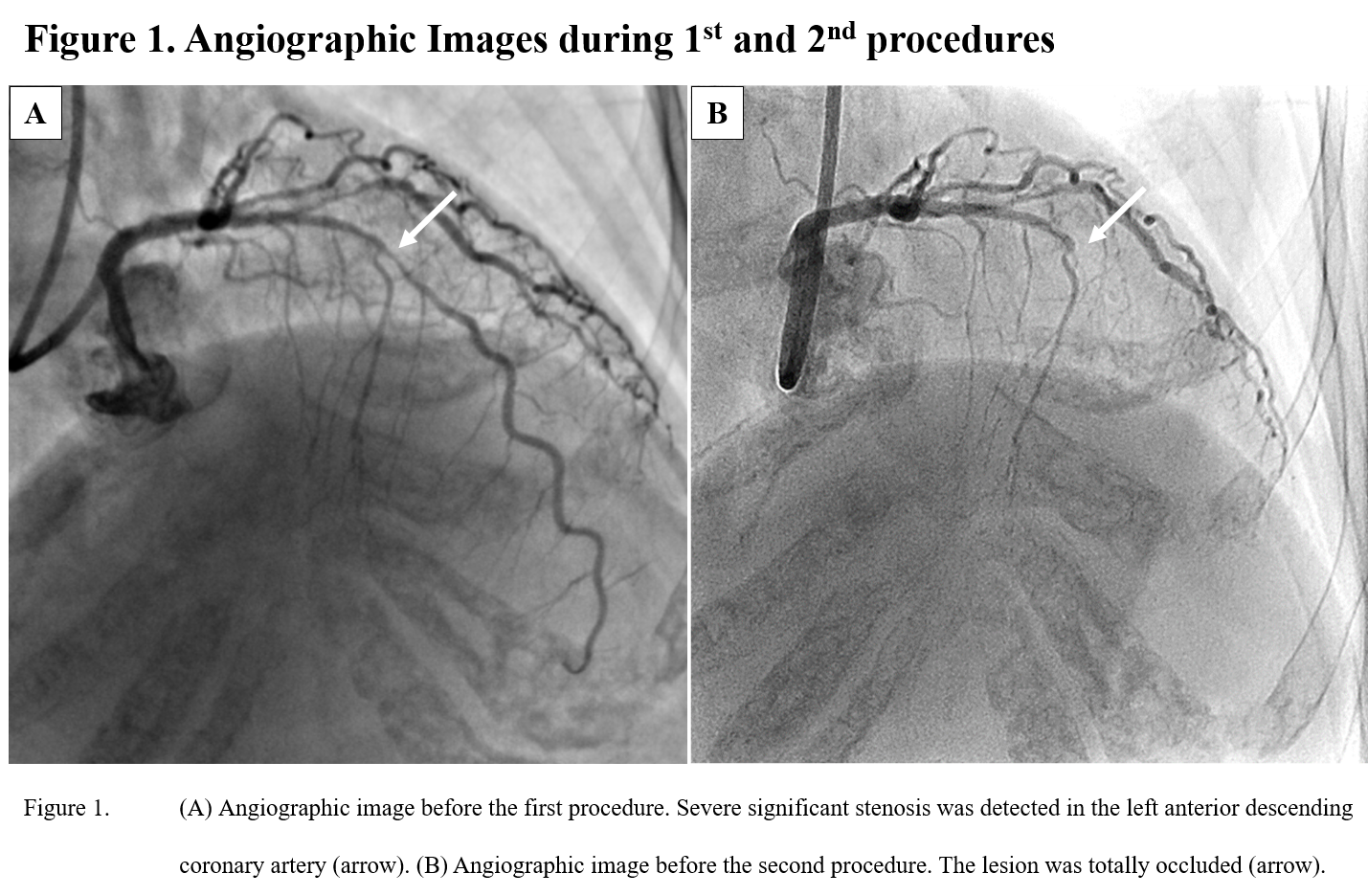 -Relevant test results prior to catheterization:
Echo cardiography showed existence of asynergy from anteroseptal to apex at previous hospital.ECG showed inverted T wave at V2-V6.
- Relevant catheterization findings:
Right coronary angiography looked normal. Left coronary angiography showed severe stenosis due to calcification in the middle of left anterior decending artery at previous hospital in February 2019. The stenosis became to occlusion when we confirmed by angiogram at our institution in April.
|
|
|
[Interventional Management]
- Procedural step:
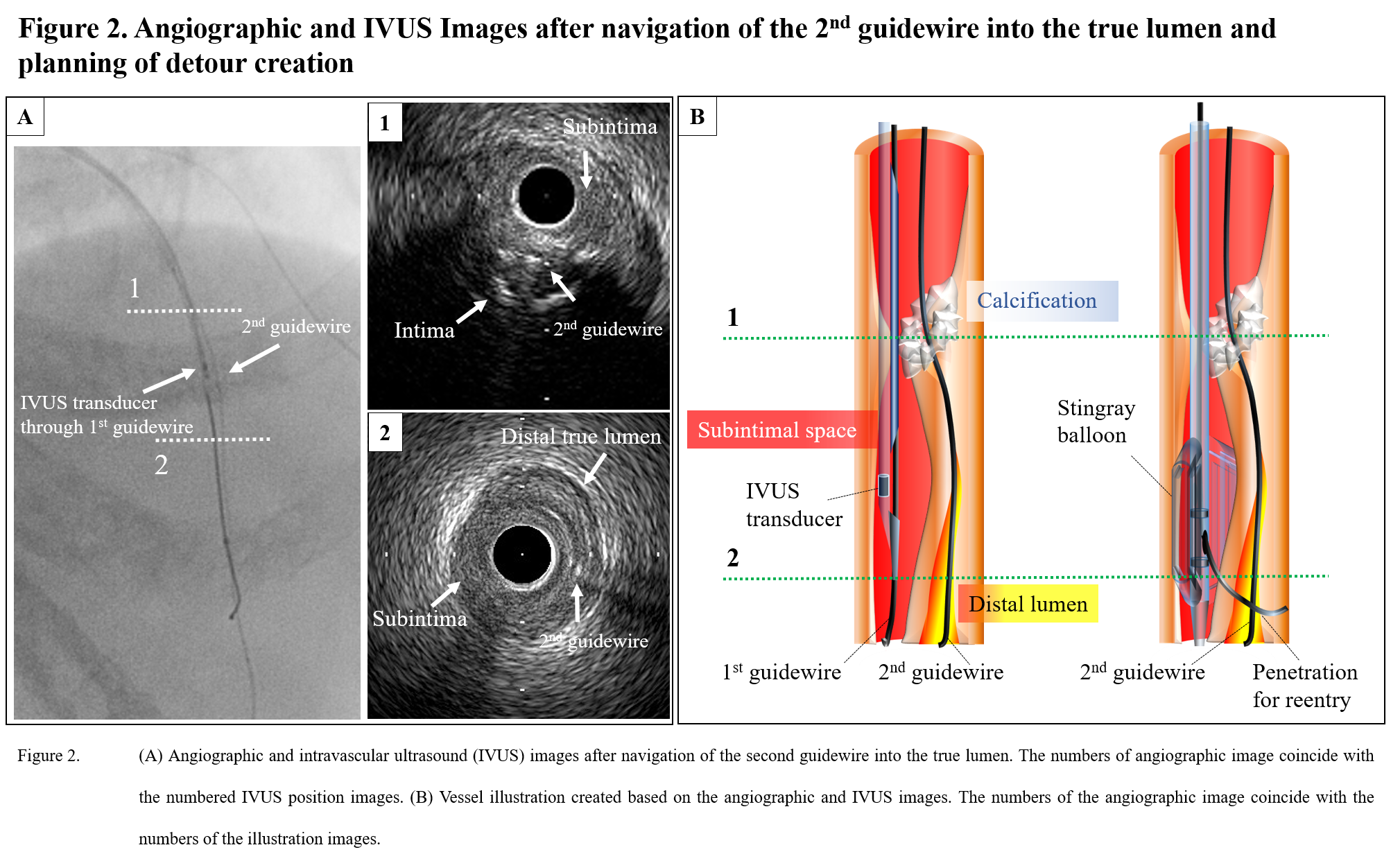
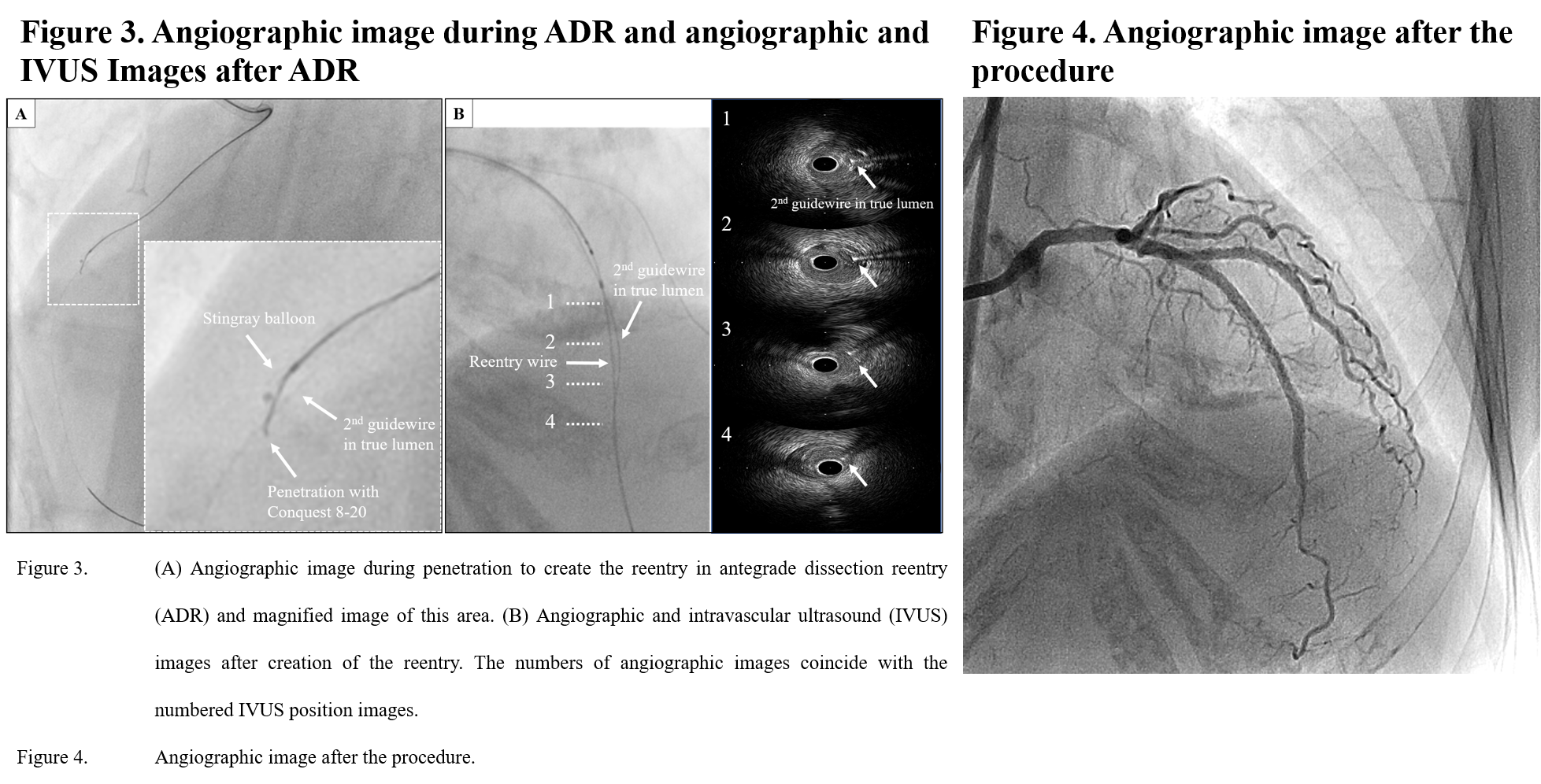
An 8-Fr left Judkins-3.5 guide catheter (Medtronic AVE, Santa Rosa, CA) and a 7-Fr left Amplatz-1.0 guide catheter (Medtronic AVE) were engaged into the left and right coronary arteries, respectively, through the bifemoral arteries. There were no visible interventional collaterals and the entrance to the CTO was located at the bifurcation site of a small septal branch. Therefore, under observation using Navifocus WR intravascular ultrasound (IVUS) (short tip without a pullback transducer system; Terumo, Tokyo, Japan) inserted into this septal branch, the first guidewire (Ultimate Bros3; Asahi Intecc, Aichi, Japan) supported by a Corsair (Asahi Intecc) was navigated into the entrance of the CTO. As the Ultimate Bros3 seemed to enter the subintimal space, AltaView IVUS (long tip with a pullback transducer system; Terumo) was advanced through the Ultimate Bros3, which showed that the first guidewire had entered the subintimal space 0.5 mm distal from the entrance of the CTO because of severe calcification. The second guidewire (Confianza-12g; Asahi Intecc) supported by the Corsair was advanced and IVUS-based 3D wiring using the tip detection method (2) allowed accurate advancement of the Confianza-12g to the true lumen (Figure 2A).However, balloons and microcatheters could not be passed through the occluded lesion due to severe calcification even using the balloon anchoring technique at a diagonal branch. The route of the extremely compressed true lumen (Figure 2A-2) may have been lost if the Confianza-12g had been changed to a Rota guidewire without using microcatheters. As the severe calcification was only 1 cm in length, we decided to perform ADR to make a detour and avoid the area of severe calcification (Figure 2B). Using IVUS, the reentry point was decided as close as possible to where the true lumen had collapsed but was fixed to the media at 180° to ensure a higher penetration range (Figure 2A-2). The first guidewire (Ultimate Bros3), which was located in the subintimal space, was changed to a Miracle 12 guidewire (Asahi Intecc), and then a Stingray balloon was inserted into the subintimal lumen. As the reentry point was compressed and could not be visualized by angiography, the second guidewire (Confianza-12g) located in the true lumen was used as a marker of the true lumen. Reentry was successfully created by the first deep penetration of a Confianza-8-20g through the distal exit of the Stingray balloon (Figure 3A). An XT-R guidewire was advanced through this reentry route and IVUS showed that ADR successfully created a 1.5-cm detour to avoid the calcification (Figure 3B). The CTO lesion was dilated with two drug-eluting stents. Only two small septal branches were occluded due to the creation of the detour and normal antegrade blood flow was achieved (Figure 4). There was no evidence of elevated creatinine-kinase level the day after the procedure and the patient was discharged on day 3 after PCI.
  - Case Summary:
ADR is usually used to pass through CTO lesions by creating a reentry from the subintimal space when the guidewire has entered into the subintimal space. In the present case, we applied the ADR technique to create a detour in a calcified CTO lesion impassable to devices after passage of the guidewire. The first guidewire entered the subintimal space and the second guidewire (Confianza-12g) was passed through the true lumen by IVUS-based 3D wiring. Therefore, the route of the compressed true lumen may have been lost if the second guidewire had been changed to a Rota guidewire without using microcatheters.There were several technical points of note in the present case. As the second guidewire located in the true lumen was used as a marker of the true lumen, angiography was not necessary to determine the penetration direction in creation of the reentry. The IVUS catheter was already inserted into the subintimal space to navigate the second guidewire into the true lumen. Therefore, IVUS observation was also performed to determine the optimal reentry point. The reentry point was set as close as possible to where the collapsed true lumen was fixed to the media around 180° so that there was a high penetration range with minimal branch loss. In the present case, we used two types of IVUS to navigate the second guidewire into the true lumen. Navifocus WR (short tip without a pullback transducer system) was used to observe the entrance of the CTO from the small septal branch and AltaView (long tip with a pullback transducer system) was used for IVUS-based 3D wiring. In CTO-PCI as shown in the present case, an IVUS system with both a short tip and pullback system is desirable; therefore, we produced AnteOwl WR IVUS (Terumo), with a short tip and a pullback transducer system. We began using AnteOwl WR in clinical practice in October 2019 after the present case.
|
|