Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_009
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| The Journey of a Bifurcation Lesion | |
| Md. Shariful Islam1, Mesbah Islam2 | |
| National Institute of Cardiovascular Diseases, Bangladesh1, Zia Hart Foundation And Reseach Institute, Bangladesh2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr.X
-Relevant clinical history and physical exam:
Mr. X, 60 years male, smoker, hypertensive, non diabetic, admitted to NICVD with the complaints of worsening central chest pain which correspond to CCS class-III for 3 days on the background of exertional chest pain for last 4 months
On examination: Pulse:76/min,regular;BP: 110/80 mmHg; Lung bases: clear -Relevant test results prior to catheterization:
ECG: OMI(A/S);
Echocardiography: Antero-septal wall hypokinesia, LV EF 40%; Troponin I: Not raised, RBS-5.6 mg/dl - Relevant catheterization findings:
Left main coronary artery (LMCA)- Normal
LAD: Osteoproximal 80-90 % LCX: 20-30% Osteal Lesion RCA: Normal What to do next? Is the lesion of LAD extent upto LM? Is the lesion of Lcx non-significant? Is there any need of protection to Lcx? How we protect Lcx? |
|
|
[Interventional Management]
- Procedural step:
Procedure: We decided to go femoral approach by 7F femoral sheath andselect guide cath EBU. We wire the bothLAD & LCX then a 2.0 X 10 mm sizeballoon was negotiated and it placed into LCX at 6atm, Then we predilate theLAD & LM lesion by 2.5 X 8mm at 10atm for LAD & 3 X 12mm at 14 atmrespectively, We place DES crossover stenting from LM to LAD (4X 28 mm for LM & 3 X 38 mm for LAD).During stent implantation LCX balloon also inflated. Then post-dilatation was done. Before crossover stentingfor LM to LAD IVUS was done. After stent implantation we again did IVUS. FinalCAG showed both the stent properly dilated, no residual stenosis with TIMI-3flow.
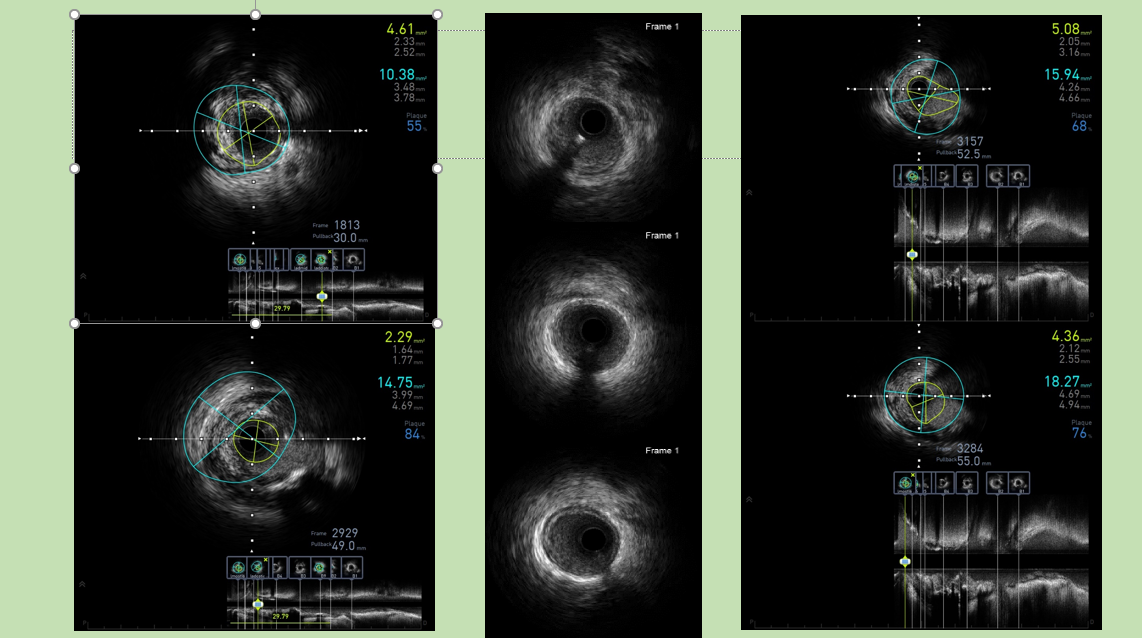 - Case Summary:
Bifurcation lesions are common in modern PCI.
There are many bifurcation technique. Choose based on anatomic and other clinical variable. Understand novel professional strategies including the jailed-balloon technique. IVUS can guide optimal placement of stents and verify appropriate expansion in the neocarina and mandatory for LM PCI |
|