Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_005
| ENDOVASCULAR - Carotid & Neurovascular Intervention | |
| How We Do It: Acute Stroke Intra-Arterial Thrombectomy in a Post-CABG Patient | |
| Tao-Ming Chen, Chun Kai Chen3, Shih Wei Meng3, Ming-Hsien Lin, Mu-Yang Hsieh3 | |
| , National Taiwan University Hospital, Taiwan3, | |
|
[Clinical Information]
- Patient initials or identifier number:
HH1111, Mr. Huang
-Relevant clinical history and physical exam:
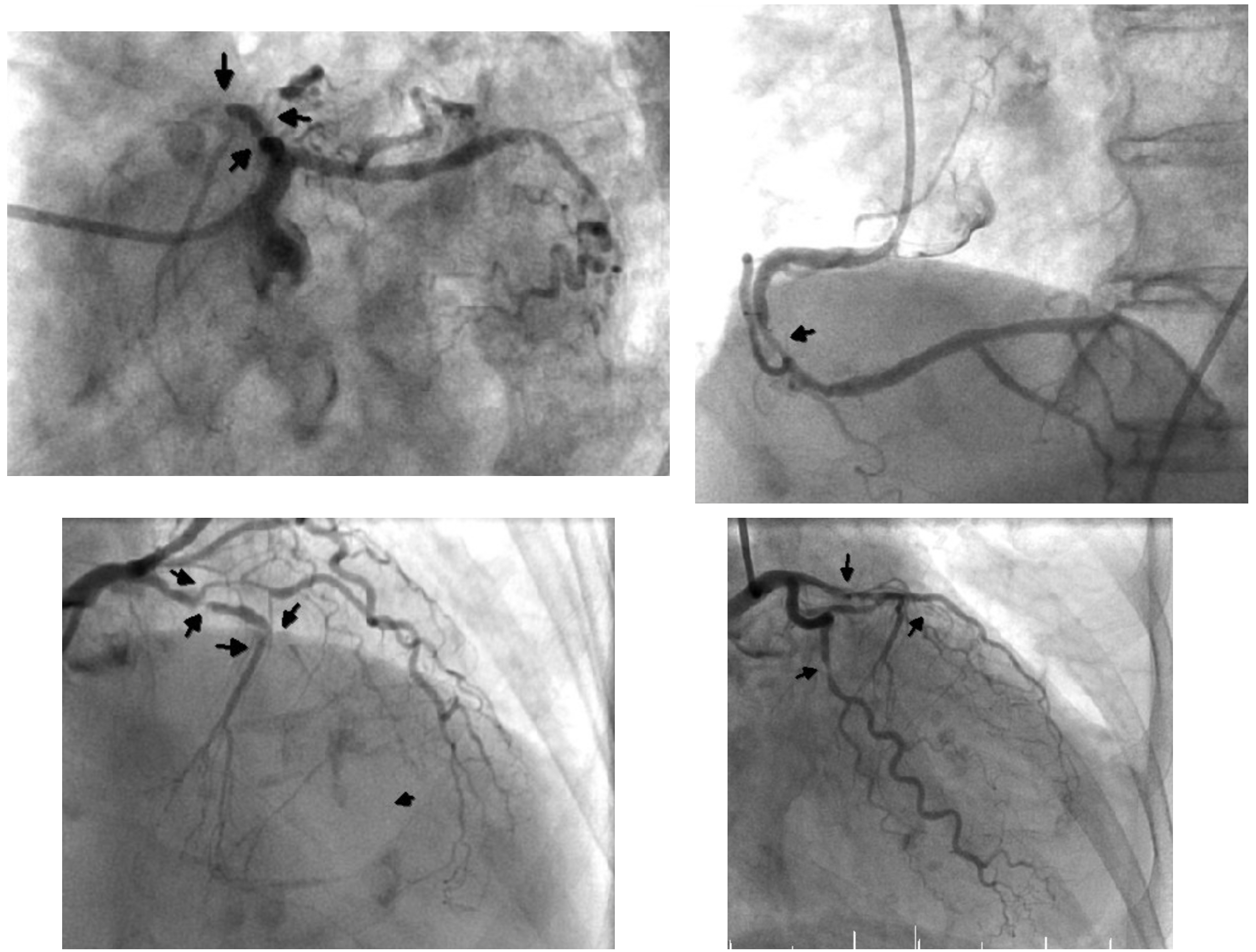
A 82-year-woman presented with non-ST elevation myocardial infarction. An urgent coronary angiography disclosed 3-vessel-disease and the patient received CABG. At post-CABG day 6, the patient developed paroxysmal atrial fibrillation. After amiodarone infusion (150 mg iv drip) the rhythm was converted to sinus rhythm. The patient had no symptoms until post-CABG day 8, when acute left hemiplegia developed. The symptoms had fluctuated over the next 8 hours.
 -Relevant test results prior to catheterization:
Emergent brain perfusion CT found large penumbra in the MTT (mean transit time) series. The infarct core was small by brain perfusion CT CBV series (cerebral blood volume). CT angiography confirmed total occlusion at distal M1 segment of the Rt MCA (middle cerebral artery). 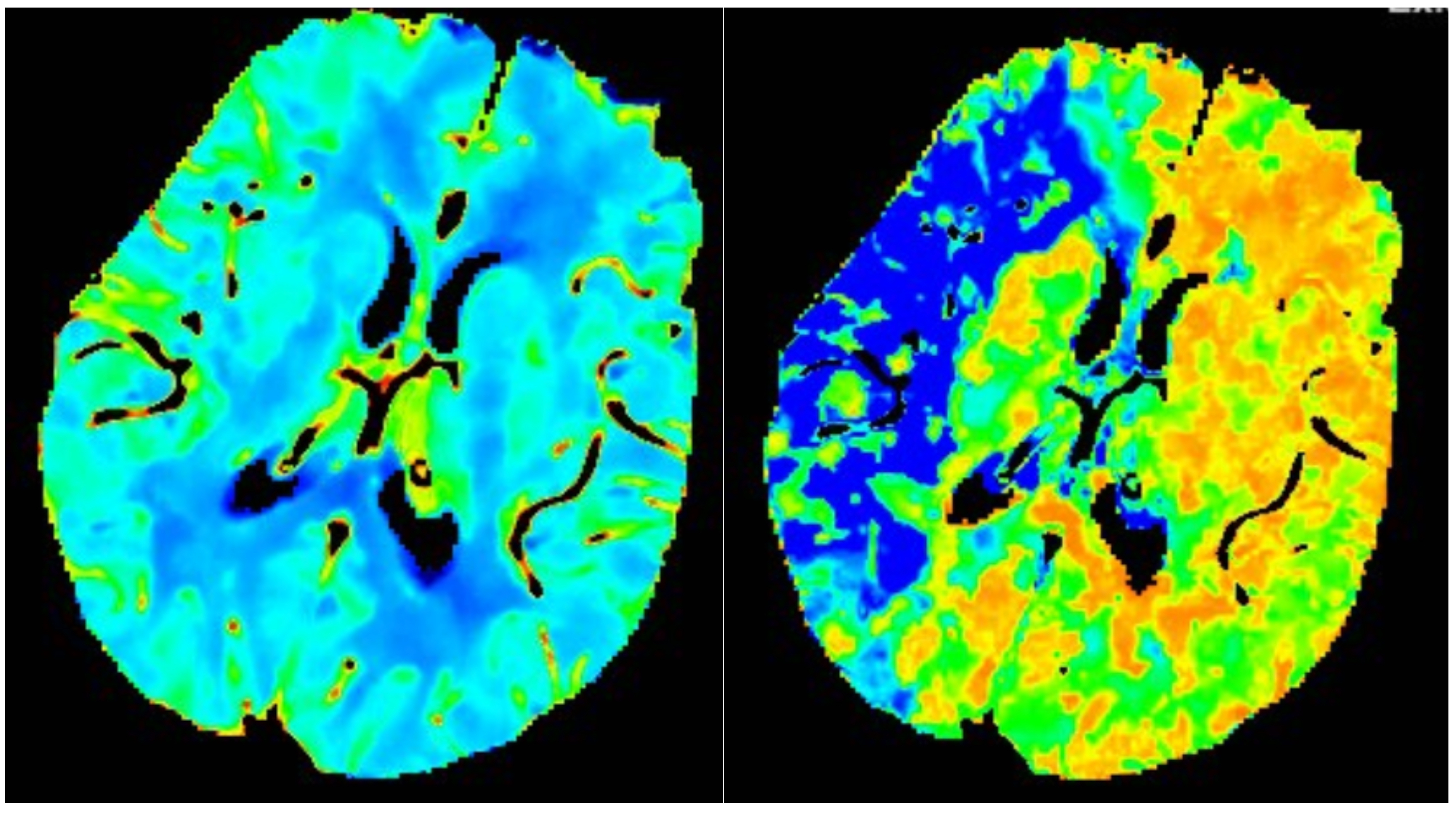 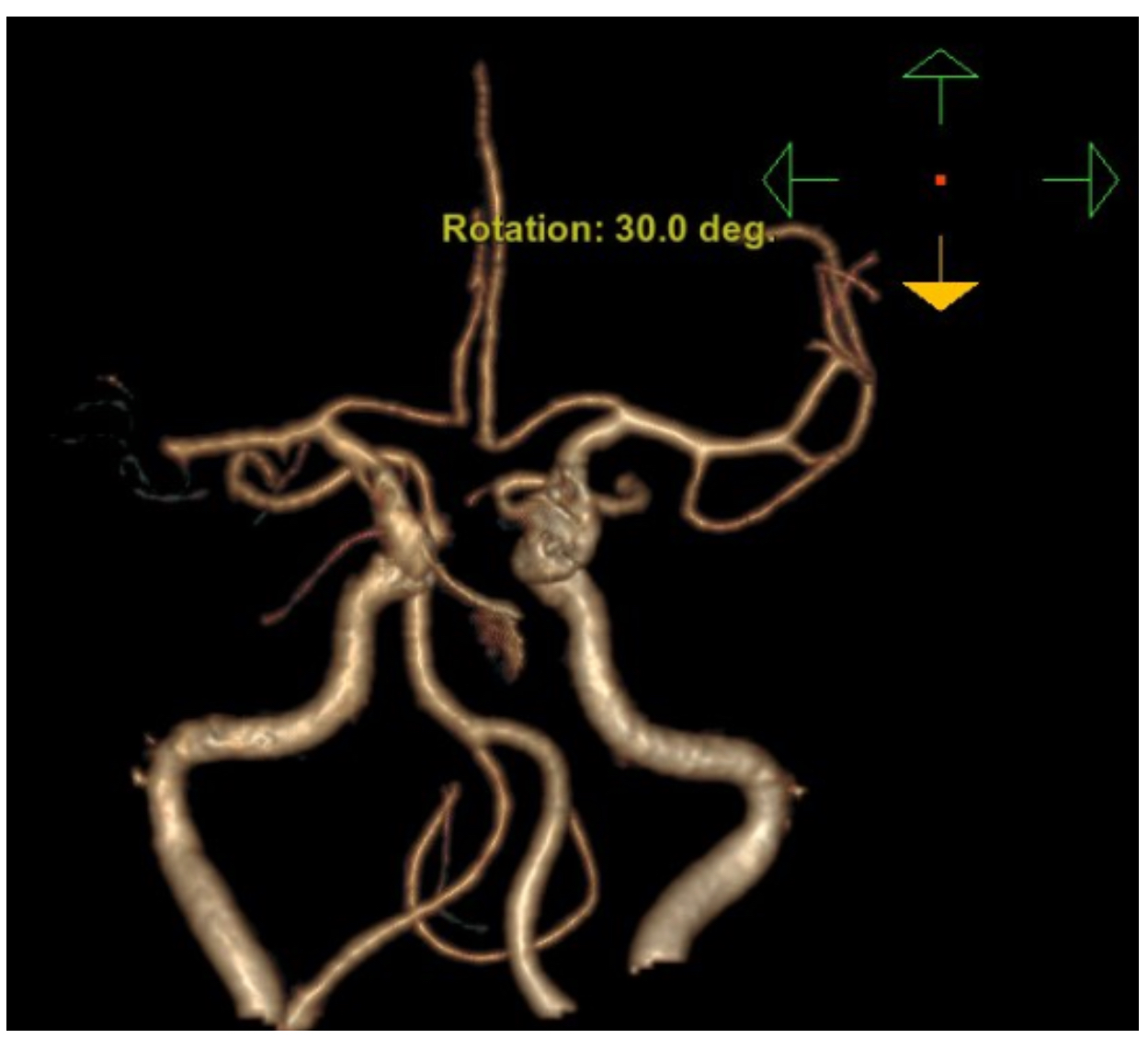 - Relevant catheterization findings:
Emergent carotid and cerebral angiography: a thrombus was identified at the distal segment of Rt MCA M1. 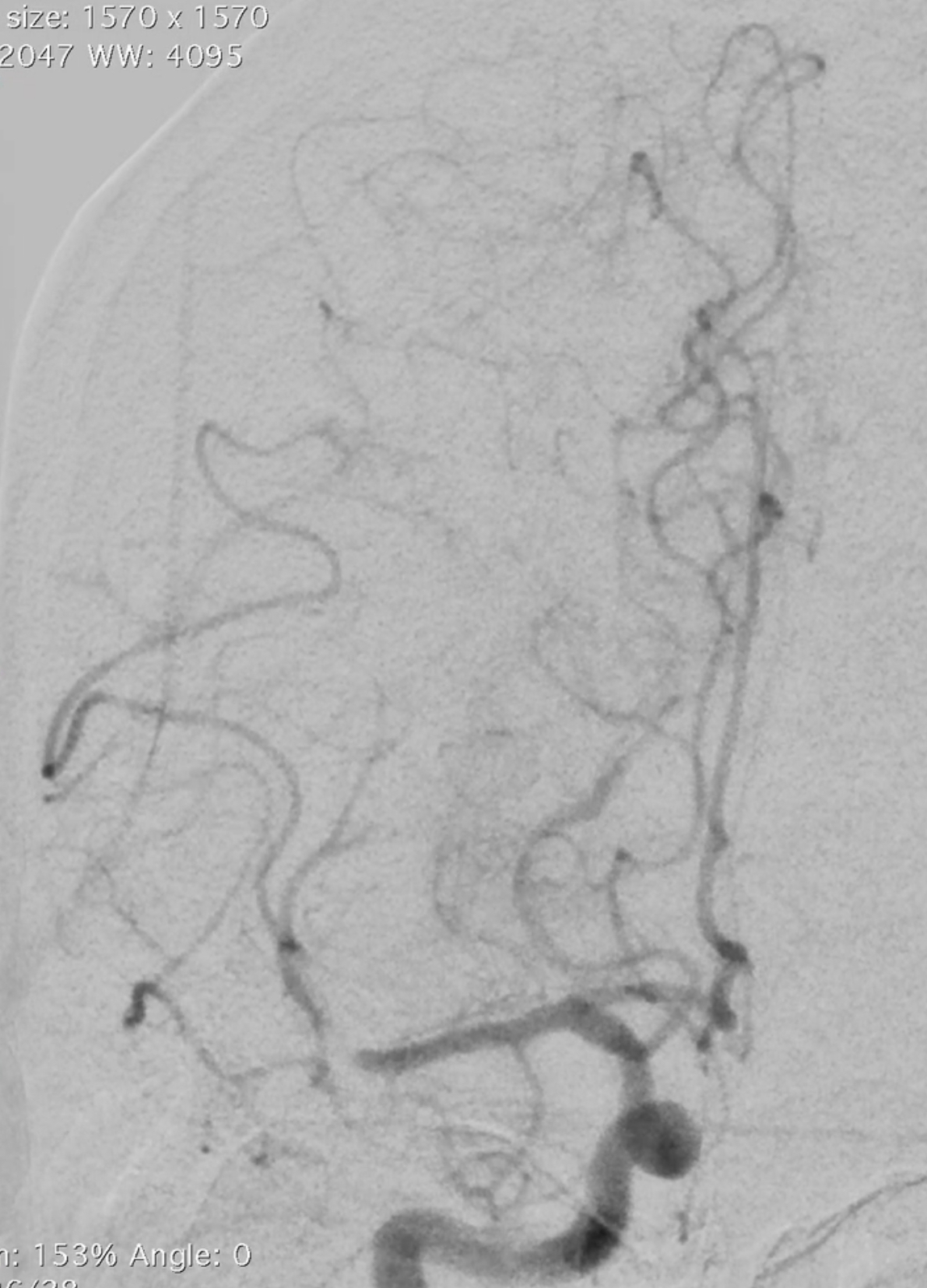 |
|
|
[Interventional Management]
- Procedural step:
1. Rt CFA puncture with ultrasound-assistance (with Merit micro-puncture kit- 4Fr). 2. Change sheath to 9 Fr 10 cm. 3. Bi-axial system with outer guide sheath (NeuroMax 088 90 cm) and JR4 5 Fr 125 cm. Parked the NeuroMax 088 tip at Rt ICA petrous part). 4. Tri-axial system with NeuroMax088/Penumbra 5Max ACE/Penumbra 3Max (outer/middle/inner catheters) place the tip near the thrombus. 5. Remove inner catheter (Penumbra 3Max). Use the 5Max ACE to aspiration. Activate the thrombus aspiration system (Penumbra) for 90 seconds. 6. TICI 3 flow re-established, with thrombus aspiration successful on the 1st pass (with 5Max ACE thrombosuction). 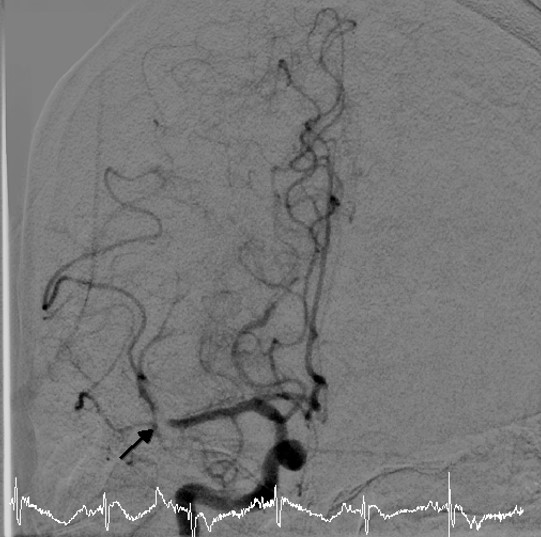 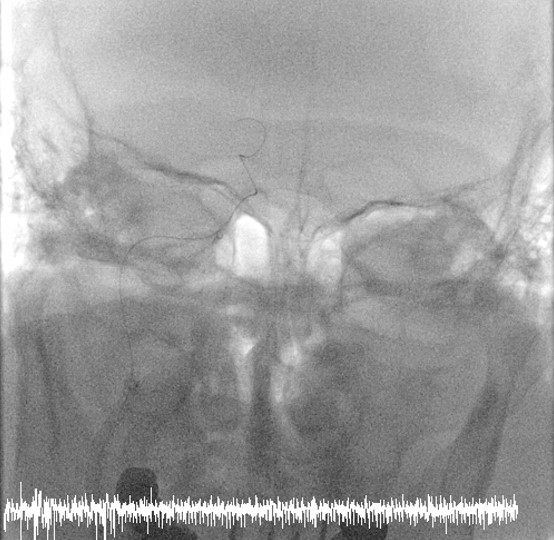 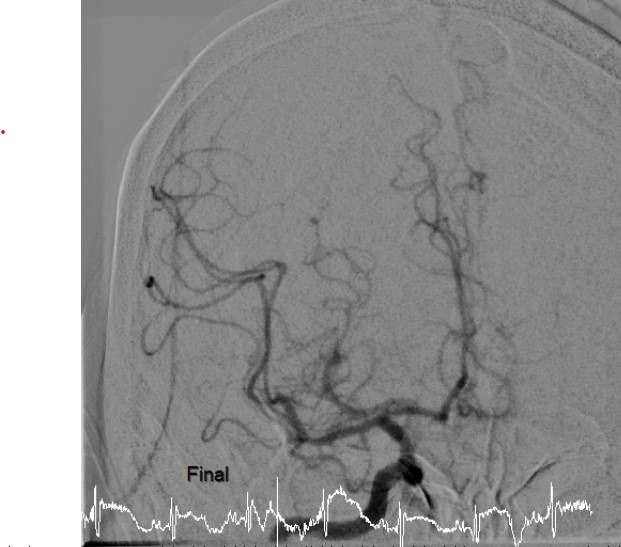 - Case Summary:
Emergent stroke IA thrombectomy in patients presented with large vessel occlusion is a proven therapy. For patients with post-CABG stroke and contraindications to systemic thrombolysis (IV rt-PA), IA thrombectomy is a reasonable alternative. For regions with limited available interventional radiologist, interventional cardiologist may fill the gap to provide best medical care.
|
|