Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191029_016
| STRUCTURAL HEART DISEASE - Valvular Intervention: Mitral or Tricuspid | |
| Successful MitraClip® Procedure for Severe Ischemic Mitral Regurgitation During the Acute Phase of Acute Myocardial Infarction | |
| Keigo Miyajima1, Shunsuke Kubo1, Koya Okabe1, Katsuya Miura1, Hidewo Amano1, Takeshi Maruo1, Kazushige Kadota1 | |
| Kurashiki Central Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
J.M
-Relevant clinical history and physical exam:
An 84-year-old woman presented to hospital with fatigue and dyspnea. Subsequently, she suffered cardiopulmonary arrest. After return of spontaneous circulation by resuscitation, she diagnosed as acute myocardial infarction and transferred to our hospital. Coronary angiography revealed three-vessel disease. We performed complete revisualization with percutaneous coronary intervention. However, it was difficult to control congestive heart failure due to severe ischemic mitral regurgitation (MR).
-Relevant test results prior to catheterization:
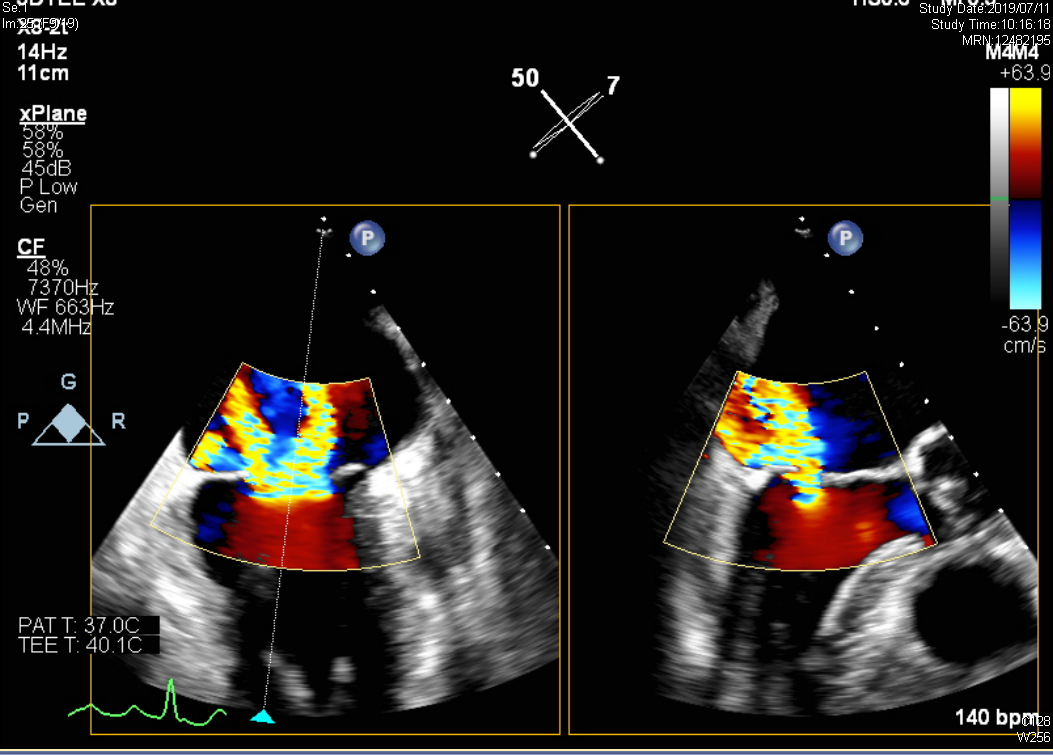
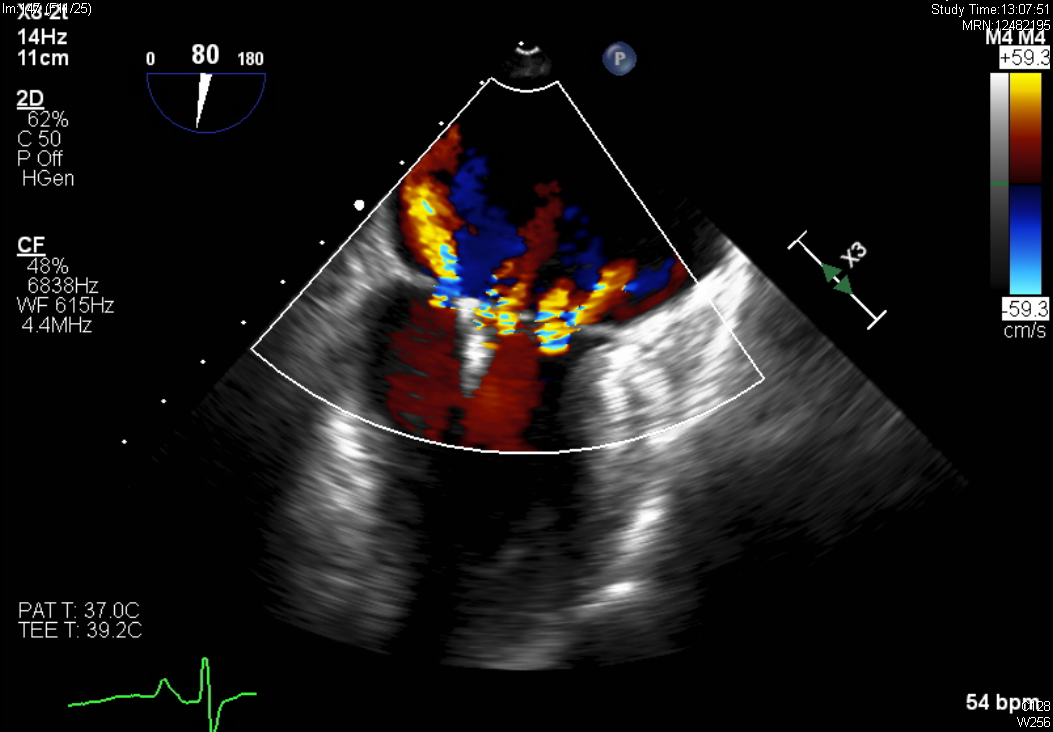
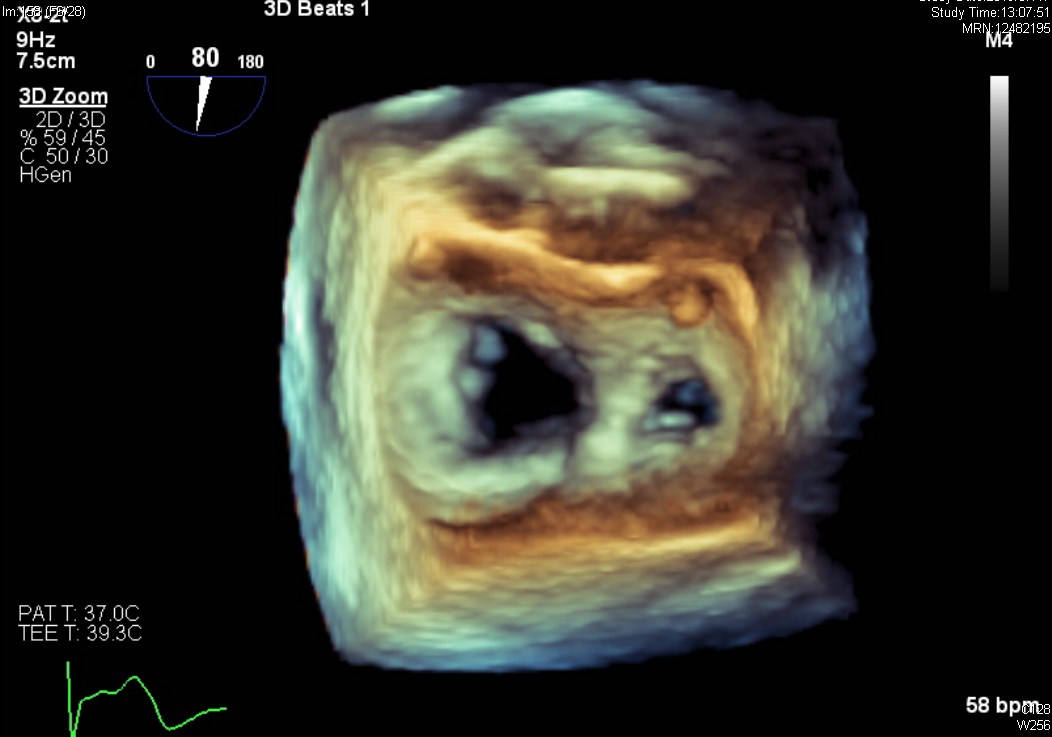
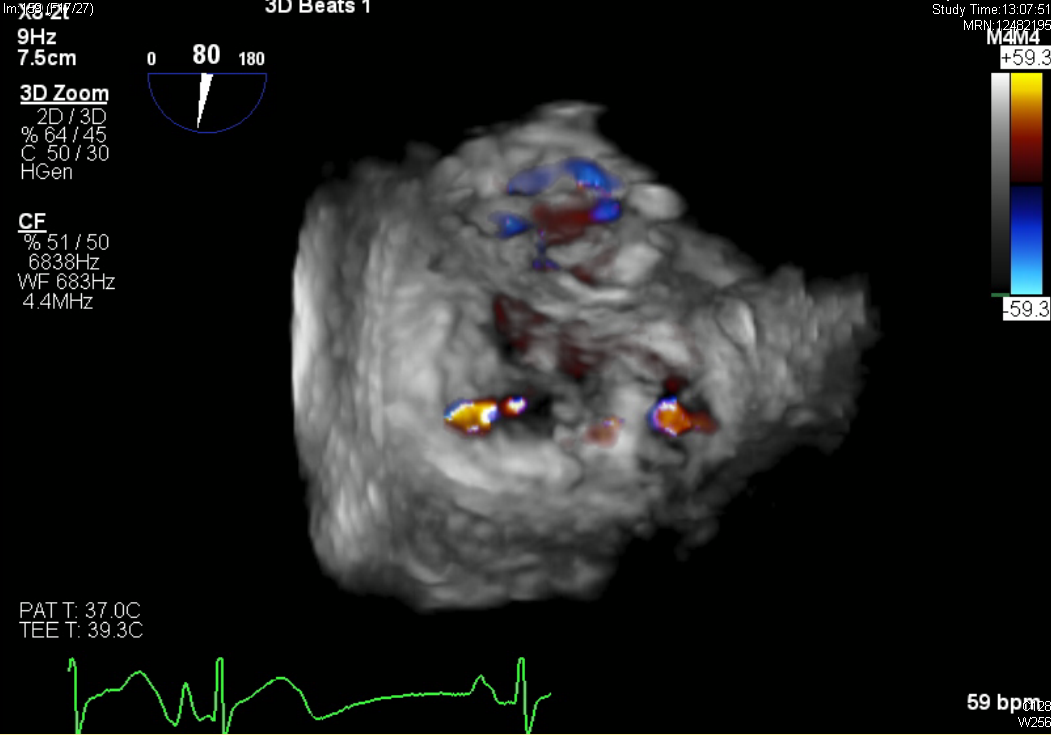
Effective regurgitant orifice (EROA) was 0.74cm2 indicating severe MR. Mitral valve orifice area was 4.38 cm2 suggesting the risk of mitral stenosis with multiple clipping. Transesophageal echocardiography (TEE) showed wide central MR jet coming from A2/P2 area. MR jet was eccentric posteriorly due to the posterior leaflet tethering associated with the posterior wall motion abnormality.
 - Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
Because patient was elderly and still in the acute phase of acute myocardial infarction, her surgical risk seemed to be high. Therefore, after the heart-team discussion, we decided to perform transcatether mitral valve edge-to-edge repair using the MitraClip device. The MitraClip procedure was performed under general anesthesia with TEE and fluoroscopy guidance. Venous access was via the right femoral vein. Transseptal puncture was performed through an 8.5Fr SL1 sheath with a RF needle. Main MR origin site was medial side of A2/P2 leaflet, so we delivered the clip to the medial A2/P2 and tried to grasp the leaflet. After the successful grasping the enough leaflet tissue, TEE revealed mild MR with 2 mmHg of mean mitral valve pressure gradient. At same time, left atrial v wave pressure decreased from 34mmHg to 12 mmHg, therefore we finished the procedure without adding a clip. After the MitraClip procedure, her symptoms markedly improved and she discharged on day 45 (post-operative day 17). At 3-month follow-up, het symptom was free with New York Heart Association class I, and TTE showed still mild MR.
   - Case Summary:
We successfully reduced ischemic MR from severe to mild using the MitraClip device during the acute phase of AMI. The gold standard therapy for ischemic MR after revascularization for AMI was optimal medical therapy. However, when heart failure associated with ischemic MR is difficult to be treated, the MitraClip is effective and less invasive therapeutic option even in the acute phase of AMI.
|
|