Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191029_003
| CORONARY - Adjunctive Procedures (thrombectomy, atherectomy, special balloons) | |
| Debulking a Diffusedly Calcified Right Coronary Artery with a Diamond | |
| Hui Beng Koh1, Nay Thu Win2, Mohamed Nazrul Mohamed Nazeeb3, Chee Sin Khaw4, Arvin Romero Yumul5, Birry Karim6, Jayakhanthan Kolanthaivelu7, Kumara Gurupparan Ganesan3, Shaiful Azmi Yahaya3 | |
| National Heart Insitute, Malaysia1, Royal Free London, United Kingdom2, National Heart Institute, Malaysia3, Sunway Medical Centre Penang, Malaysia4, Medical Center Manila, Philippines5, Cipto Mangunkusumo General Hospital, Indonesia6, Cardiovascular Sentral Kuala Lumpur, Malaysia7, | |
|
[Clinical Information]
- Patient initials or identifier number:
SBS
-Relevant clinical history and physical exam:
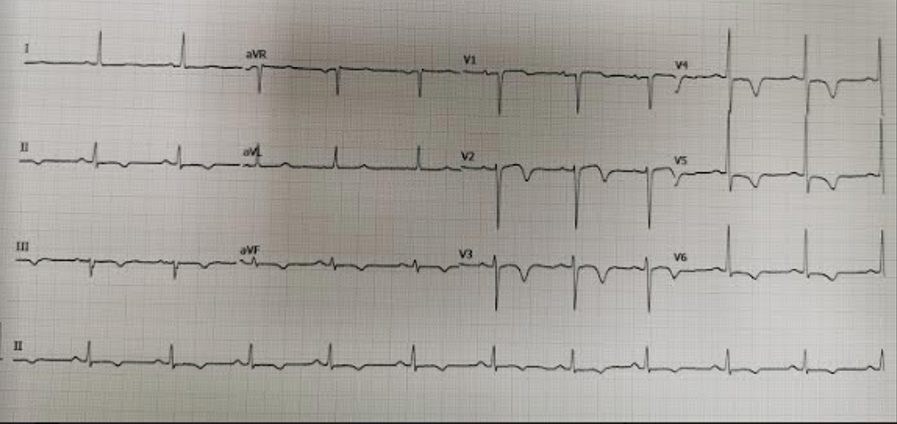
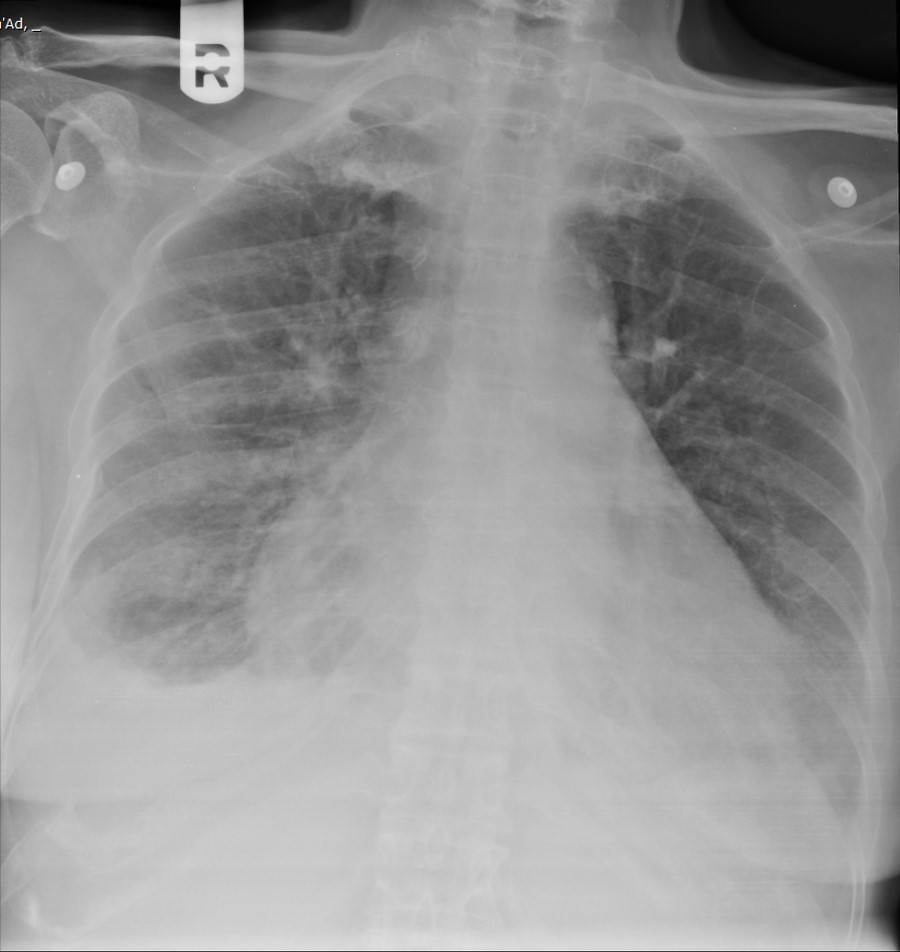
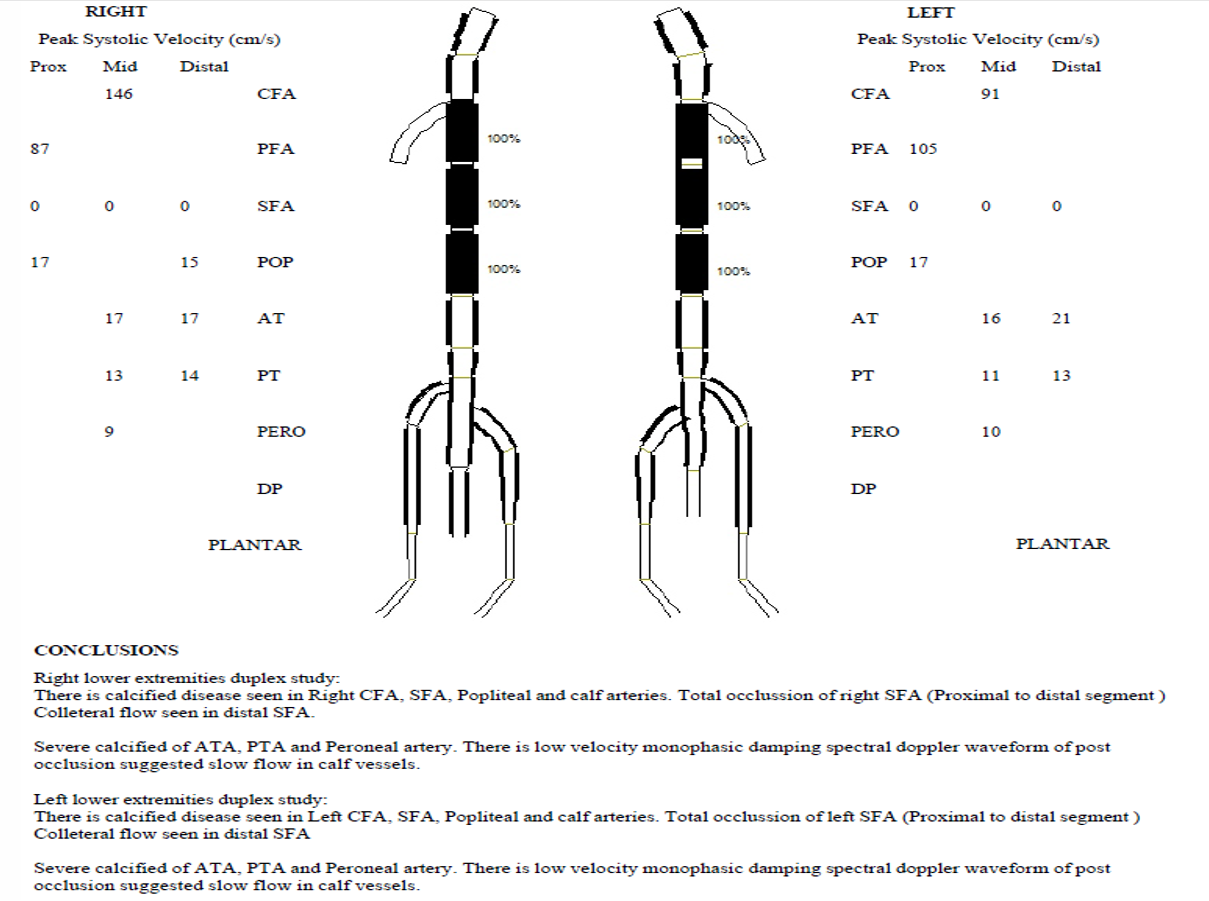
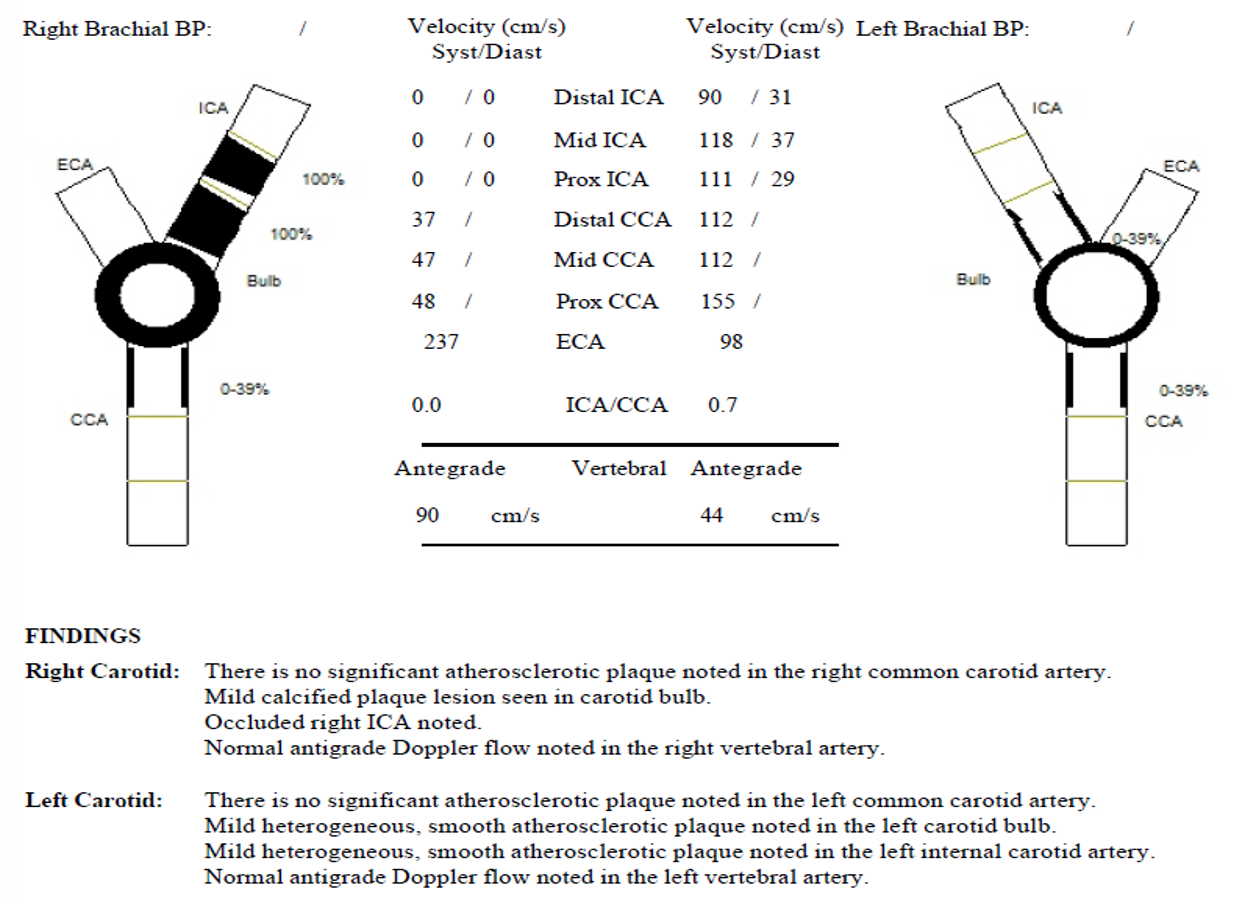
SBS is a 65 year old lady with background diabetes, hypertension, paroxysmal Afib, chronic kidney disease and history of recurrent ACS. Coronary angiogram showed severely calcified 3 vessel disease with left main (LM) involvement. She also had CTO right internal carotid artery and bilateral superficial femoral arteries. Rotational atherectomy and PCI to LM /LAD was done successfully. Planned for stage PCI to RCA. BP 120/53mmhg, HR 67bpm, Afebrile. Lungs minimal crepitations. No murmurs.
  -Relevant test results prior to catheterization:
Haemoglobin 10.6g/dLPlatelet 323 x 109 /LWhite blood cell 9.6 x109 /LFasting glucose 6.8 mmol/L Random glucose 5.5 mmol/LHbA1c 6.7% Urea 10.8 mmol/L, eGR 37ml/min/1.73m2 Creatinine 125 umol/LPotassium 5.4 mmol/LUric Acid 582 umol/LSodium 144 mmol/Lhs Troponin 34 pg/ml
   - Relevant catheterization findings:
Coronary angiogram LMS : Stent Patent LAD : Stent PatentLCx : Small, severe disease proximal OM1RCA : Calcified++, Severe disease to proximal to mid segment, severe disease distal RCA
|
|
|
[Interventional Management]
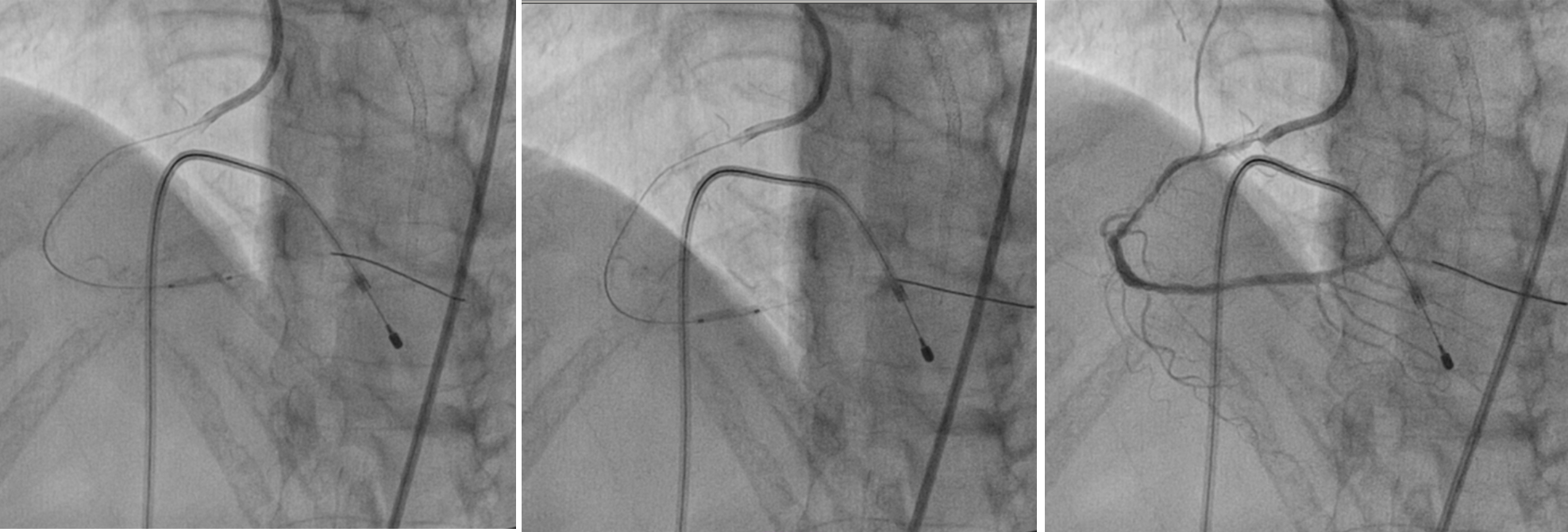
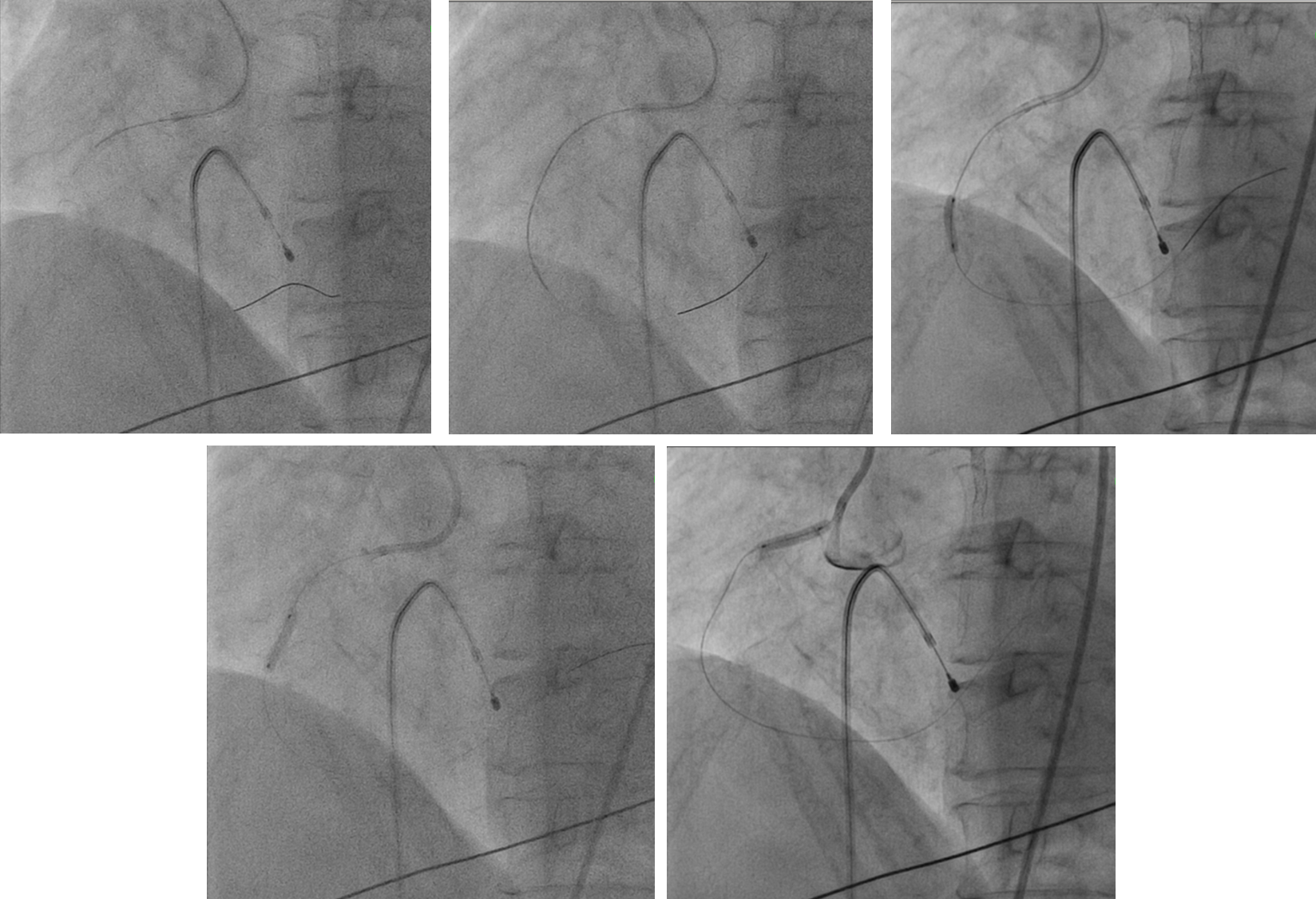
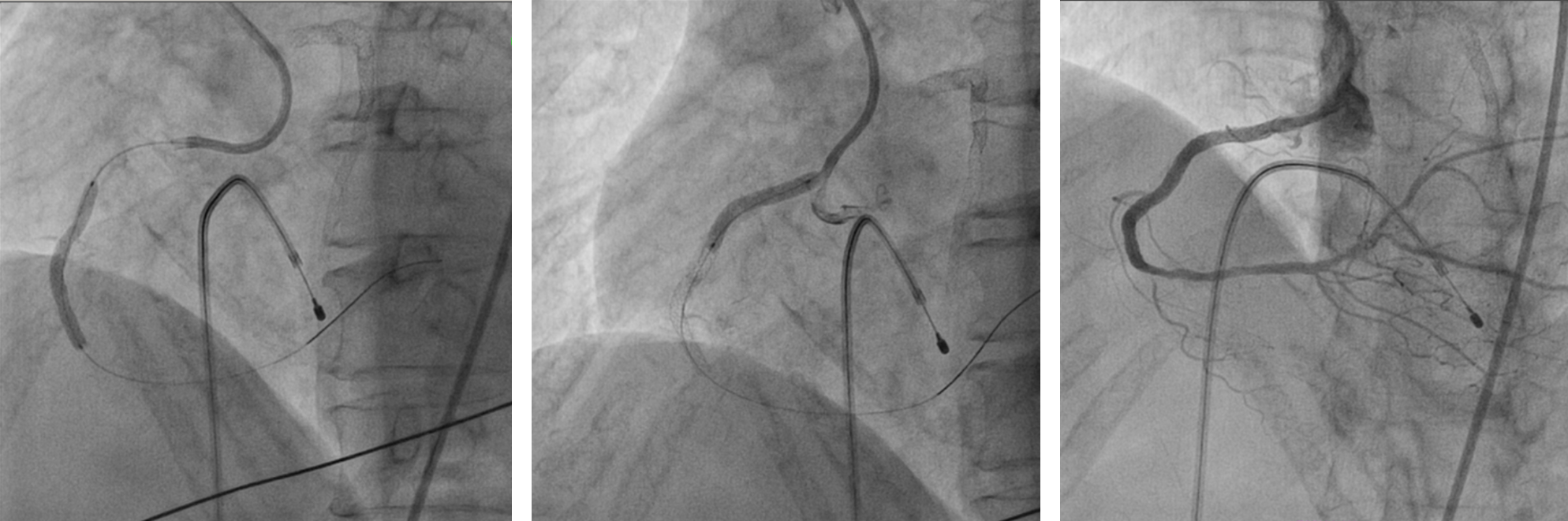
- Procedural step:
Left femoral artery punctured for Guiding catheter SAL 1.0 6F. Right femoral vein punctured for Temporary Pacemaker as back up. Wired down RCA with SION Blue and Finecross microcatheter. Exchanged SION Blue to Viperwire. Finecross removed. Predilated distal RCA with balloon 2.0/12mm at 12ATM. PTCA with Paclitaxel Coated Balloon 2.25/15mm at 6ATM. Orbital atherectomy done using Diamondback from proximal to mid segment. Exchanged Viperwire back to SION Blue via Finecross microcatheter. IVUS run done. Mid RCA size 3mm, proximal RCA size 3.5mm. Predilated mid to proximal to ostial RCA with NC balloon 2.5/15mm at 16ATM. Predilated further with NC balloon 3.0/15mm at 16ATM. Stented mid to proximal RCA with Zotarolimus eluting stent 3.0/38mm at 12ATM. Stent balloon pulled back to ostial and inflated at 12ATM. Overlap stenting from proximal to ostial RCA done with Sirolimus eluting stent 3.5/24mm at 12ATM. Post dilated with NC balloon 3.5/15mm at 12-22ATM. IVUS done, stent well opposed, MLA 7.8mm2. TIMI III flow.
   - Case Summary:
SBS was deemed unsuitable for CABG earlier in view of her co-morbidities, poor target vessels and presence of CTO over the right internal carotid artery and bilateral superficial femoral arteries. As patient was symptomatic CCS 3, NYHA 3, high risk PCI was discussed with patient. Fortunately PCI to Left main and LAD was uneventful. Stage PCI to RCA was planned. In view of heavy diffuse calcification from proximal to mid RCA, it was decided that we need to prepare the lesion well by debulking. Using Orbital atherectomy to prepare the vessel was necessary so that stents can be delivered smoothly and underexpansion of stents avoided. Using IVUS was helpful in determining the exact vessel size.
|
|