Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191029_001
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Treat True LM Trifurcation Lesion with Two Culotte Stenting | |
| Wen-Lieng Lee1, Wei-Jhong Chen1 | |
| Taichung Veterans General Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Ma
-Relevant clinical history and physical exam:
60 years old male Chief complain: anterior chest tightness for one month with recent aggravation This 60 years old male had medical history of hypertension. He suffered from intermittent anterior chest tightness, which exacerbated during exercise, in recent one month. However, the anterior chest tightness aggravation that he suffered from chest tightness even while resting. Sweating was noted while chest tightness. -Relevant test results prior to catheterization:
Troponin I 1.66 ng/ml renal function: normal EKG revealed normal sinus rhythm without specific STT change 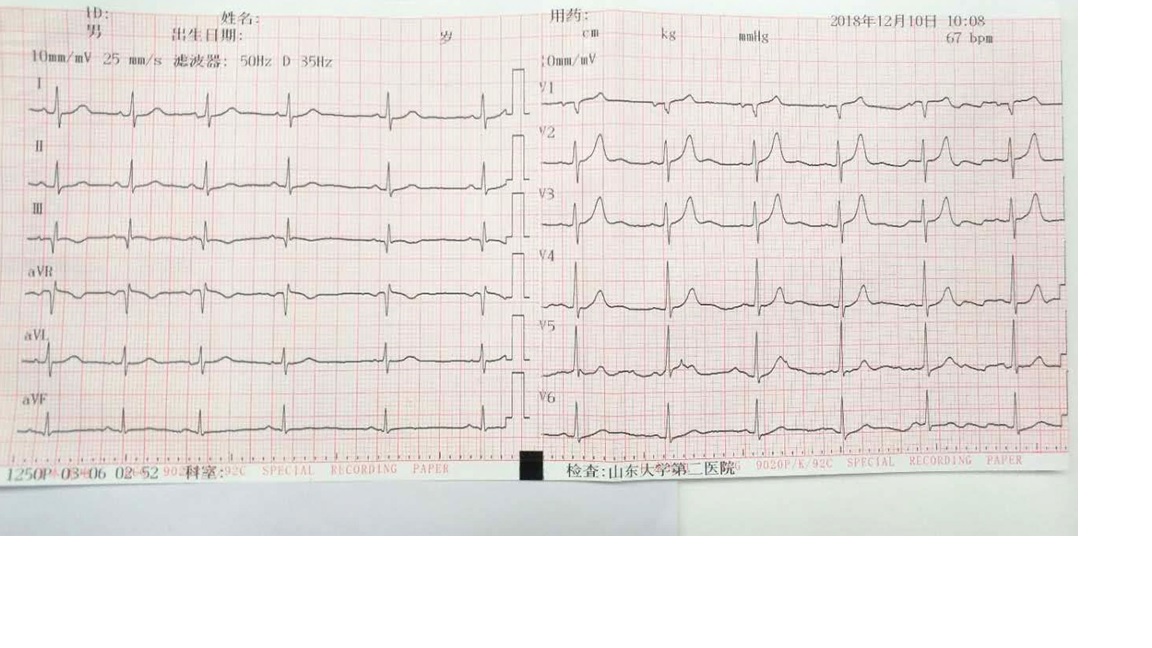 - Relevant catheterization findings:
Both side CAG revealed right dominant LM trifurcation with modified Medina 1-1-1-1 RCA artherosclerosis with patent vessel |
|
|
[Interventional Management]
- Procedural step:
Left coronary artery wasengaged by Xb guiding. Wiring LCX proper was tried first, which failed due toangulation. Thus, we had wired intermediate branch first, and then pre-dilated.Wiring LCX proper by reverse wire technique was done, successfully. IVUSfor both LCX proper and intermediate branch revealed artherosclerosis withoutcalcification at both LCX and intermediate branch ostium. Stenting for LCX-properwithout protruding to distal LM was done. Crusade-assisted rewiring intermediatewas done, subsequently. POBA for open LCX stent strut was done. We then stentedfrom distal LM to intermediate branch. Crusade-assisted rewiring LCX proper wasdone. Kissing balloon technique for LCX and intermediate branch was done. FirstCulotte was done. Wiring to LAD by Crusade assist was done with subsequent POBAfor opening stent strut. Stent was deployed from distal LM to proximal LAD. Crusade-assistedrewiring to intermediate was done with subsequent opening stent strut by POBA.Final kissing balloon technique for LAD and intermediate branch was done. Wethen POT for left main stent. Final angiography revealed TIMI-3 flow to allleft main branches, including LAD, LCX and intermediate. IVUS revealed no stentmalposition.
- Case Summary:
LM trifurcation lesions are diverse inanatomies LM trifurcation is under-reported andunder-treated in real-world practice The choice between PCI and CABG dependson multiple factors The choice between stenting strategiesdepends on the anatomies Most lesions could be solved by one- ortwo-stent strategies Three-stent strategy is most complex anddictated by coronary anatomy and SB importance Routine use of dual-lumen microcatheteris very useful by providing accurate rewiring in small working area Safety and long-term results remain theAchilles tendon of LM trifurcation PCI |
|