Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191028_018
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Non-Invasive | |
| Right Ventricular Wall Rupture Treated with an Unconventional Approach | |
| Adelyn Nisha Henry1, Gurudevan Mahadevan1, Benjamin Leo Cheang Leng2, Kumutha Gobal1, Vicknesan Kulasingham3 | |
| Sultanah Aminah Hospital, Malaysia1, Columbia Asia Hospital Tebrau, Malaysia2, Ministry of Health Malaysia, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr.J
-Relevant clinical history and physical exam:
A 67 year old gentleman was brought in to the Emergency Department. He complained of chest discomfort and shortness of breath for 2 days following which he sustained a presyncopal attack. He has history of Hypertension, Diabetes Mellitus and was an active smoker of 20 pack years. He presented about 48 hours into his symptom onset. His Blood pressure on arrival to the Emergency Department was 77/54mmhg and subsequently 95/57mmhg. He was delirious with a Glassgow Coma Score of E3V5M6.
-Relevant test results prior to catheterization:
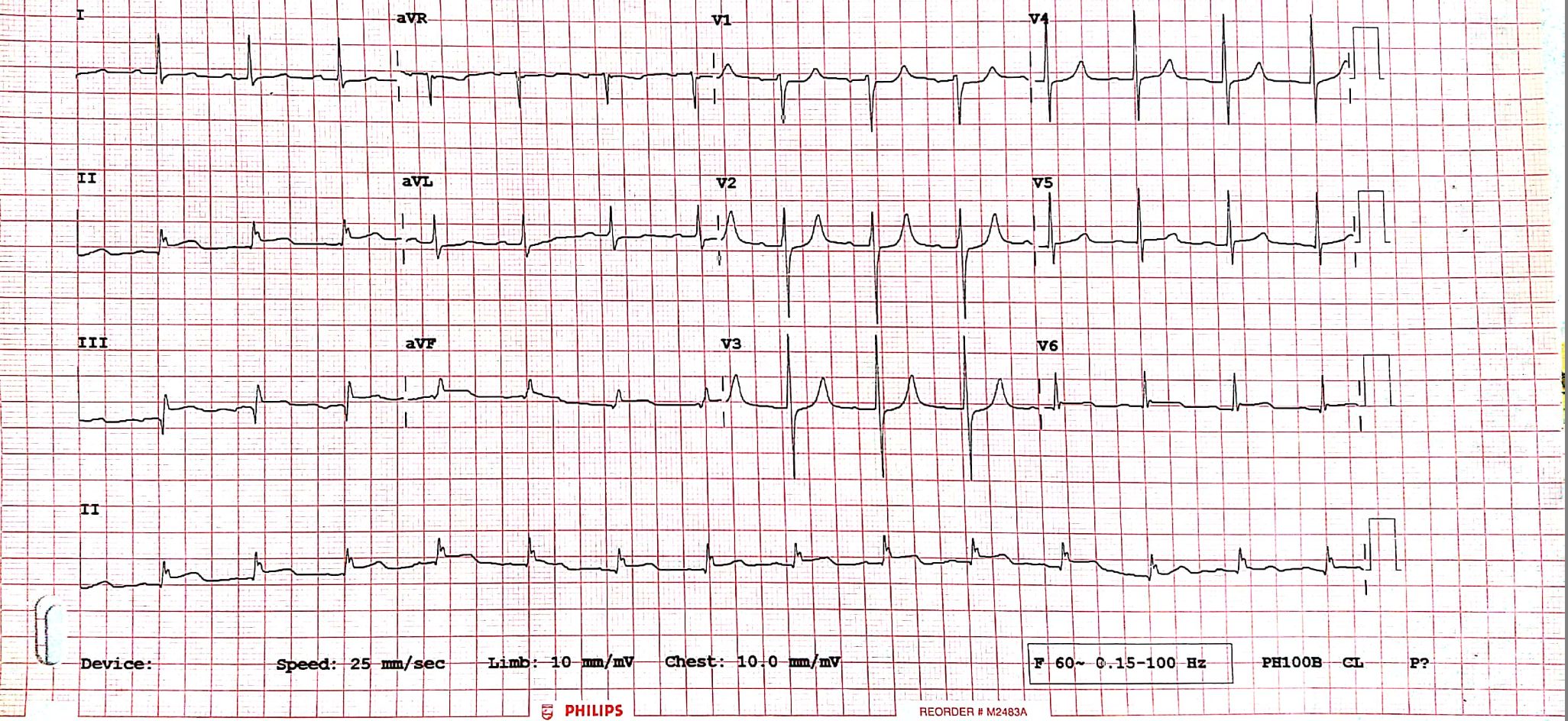
His electrocardiogram revealed St segment elevation over leads 2, 3, AVF(Figure 1).
 - Relevant catheterization findings:
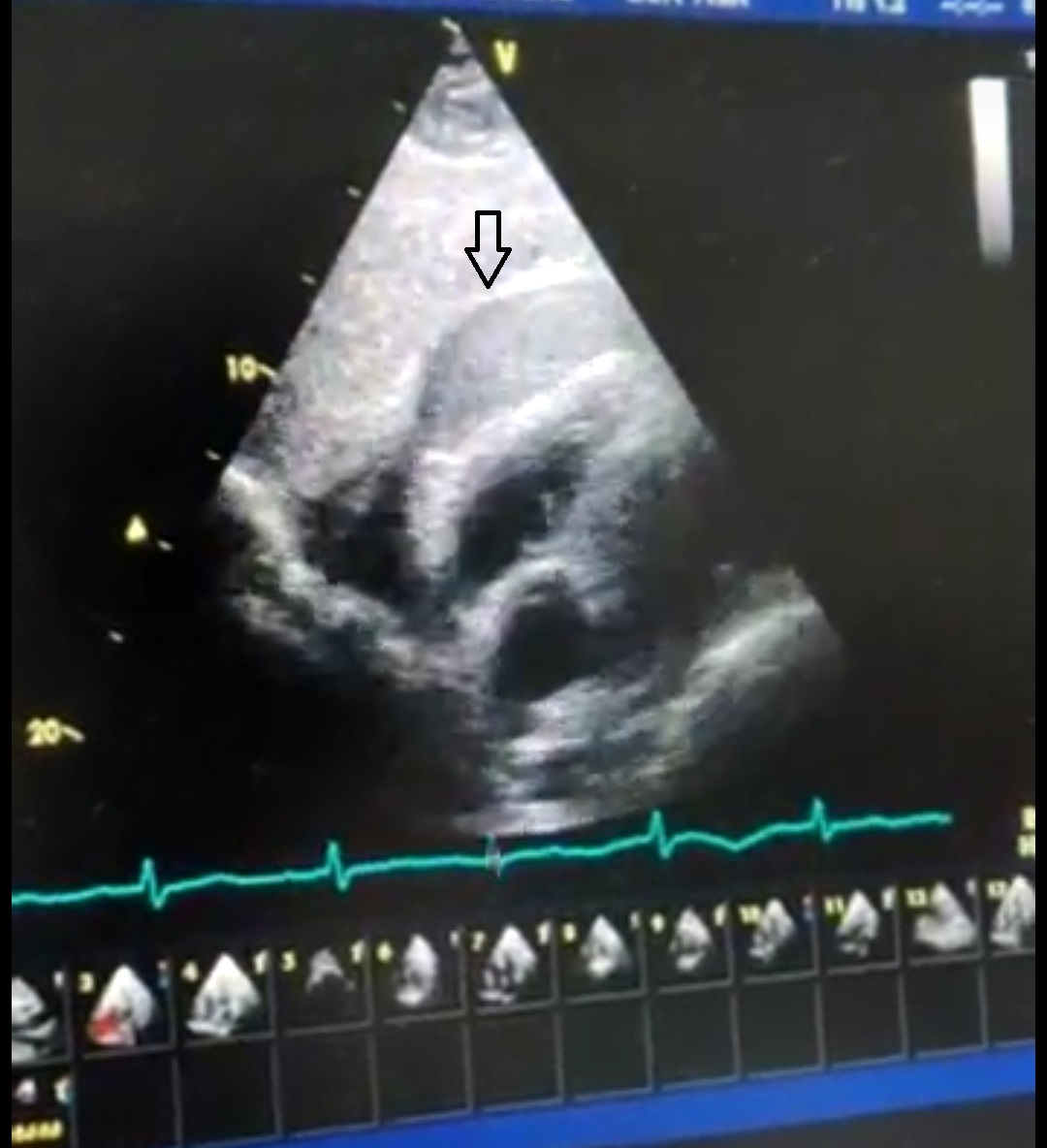
Patient was booked for Primary PCI but whilst being wheeled towards the Invasive Catheterization lab he became more confused and restless with a blood pressure of 88/55mmhg. He was pushed back into the Emergency department, started on Intravenous Noradrenaline infusion and a quick bedside echocardiogram was performed, which revealed a Right ventricular free wall rupture with a pericardial effusion and an echo dense mass along the Right Ventricular free wall(Figure 2a)
 |
|
|
[Interventional Management]
- Procedural step:
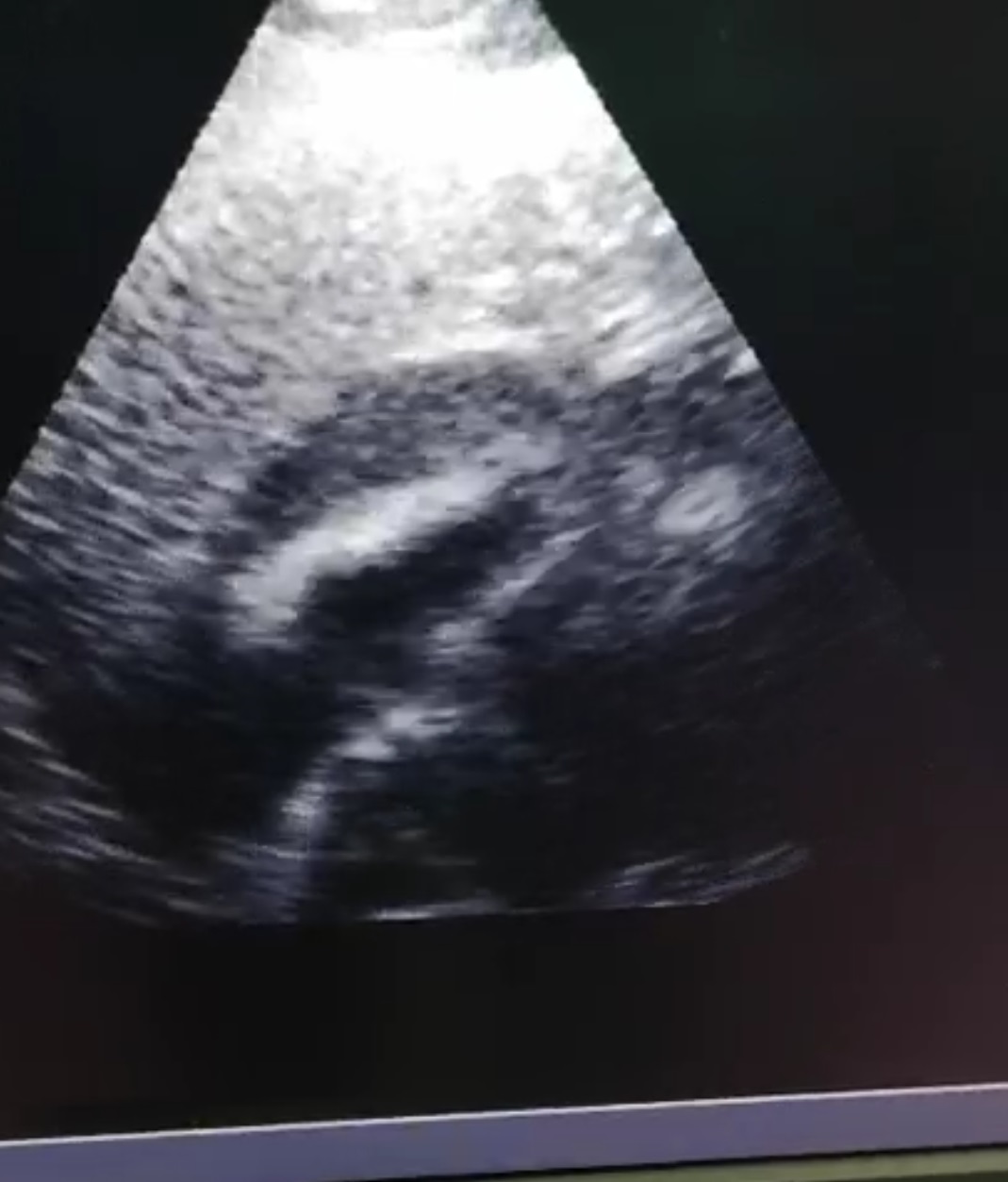
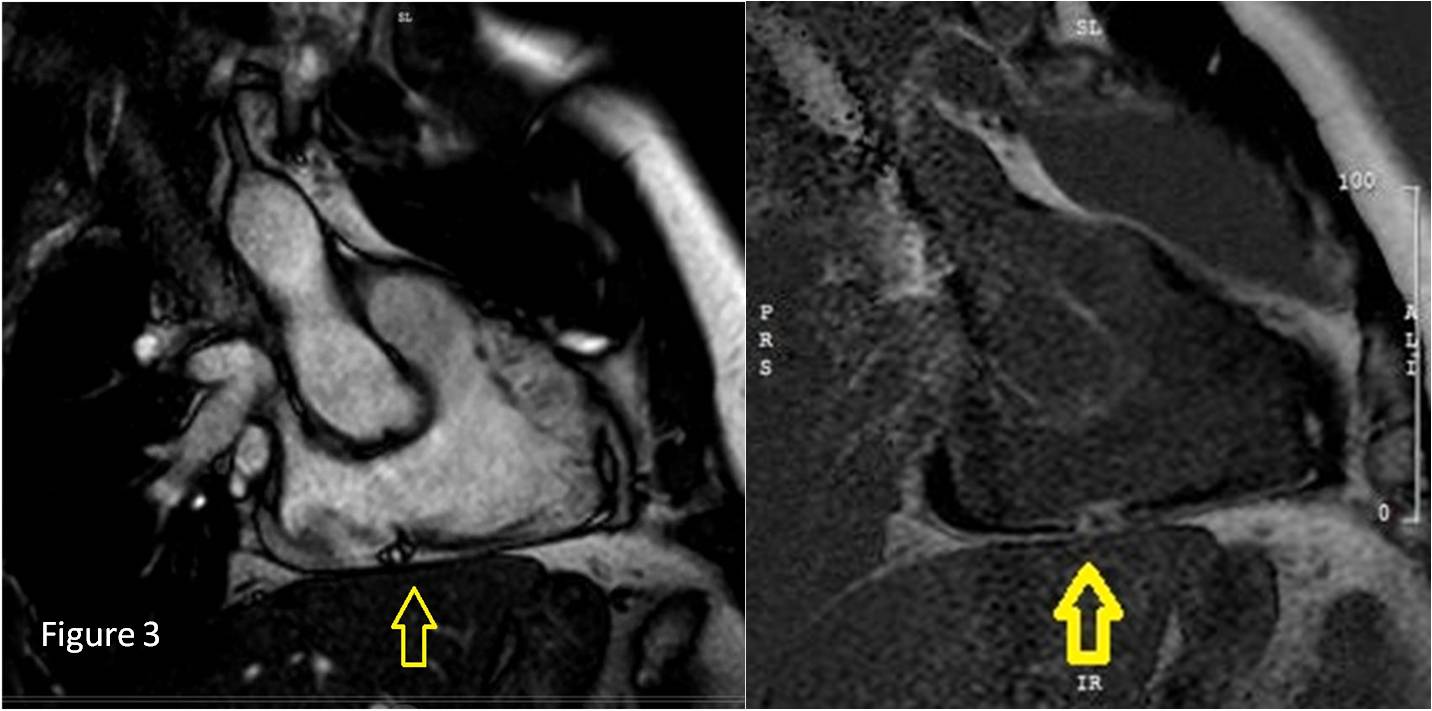
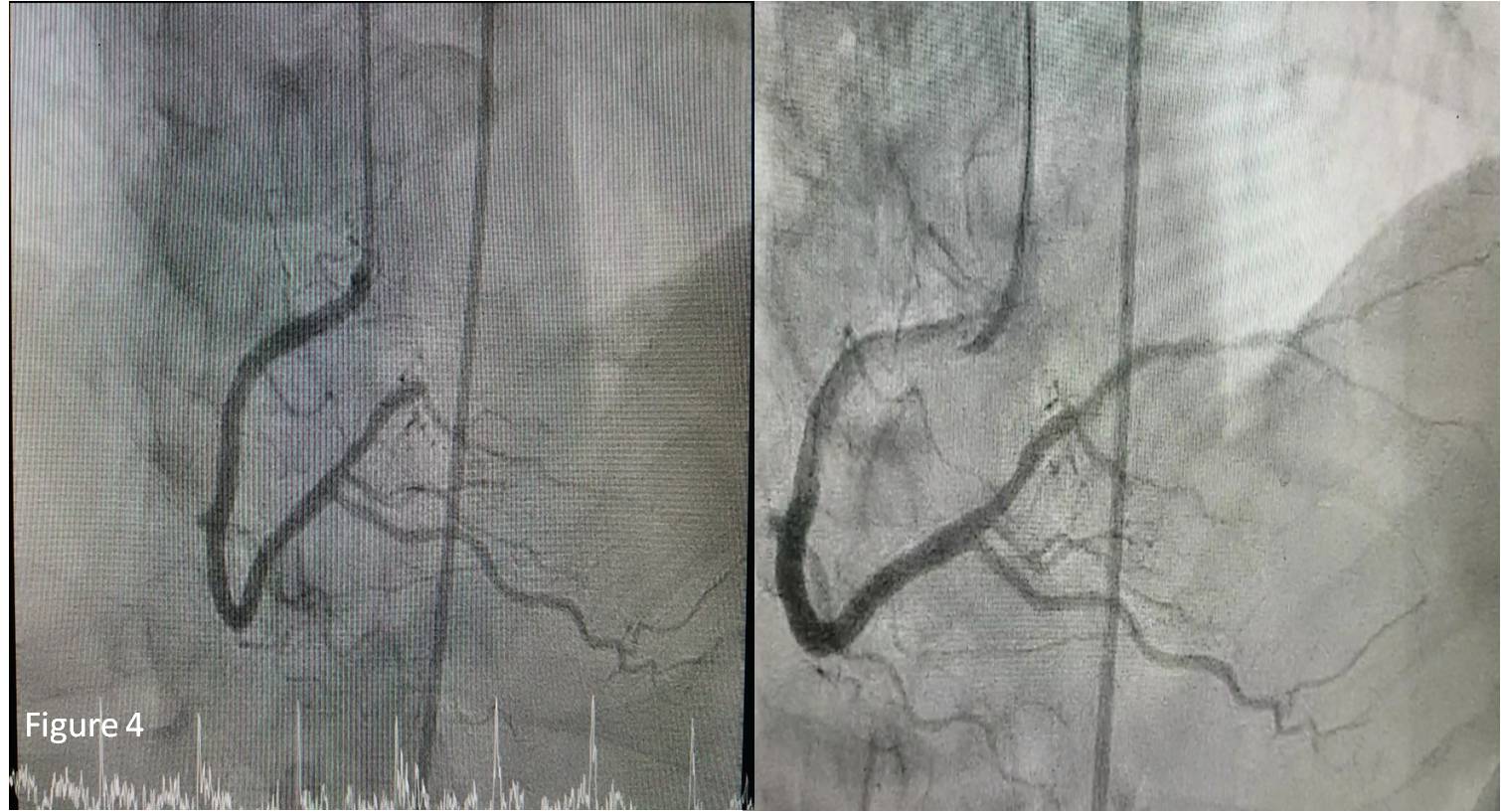
A Cardiothoracic consult was made and surgical intervention was deemed too risky for patient. Medical therapy with fluids, ionotropes with an aim to hemodynamically stabilise patient was opted for, as an initial measure. Repeat echocardiogram done the next day revealed a large pericardial effusion with absence of the echo dense mass but patient’s clinical condition remained the same. His Left ventricular ejection fraction was slightly reduced at 40-45%with inferior wall hypokinesia(Figure 2b). He exhibited no signs of raised JVP nor muffled heart sounds, blood pressure support remained static. The decision for pericardiocentasis was deferred and patient was watched carefully. A cardiac MRI was performed which revealed dyskinesia over the inferolateral segment with late gadolinium enhancement in the anterior wall of the right ventricle in keeping with prior infarction of the Left Circumflex Artery and Right Coronary Artery territory, which was viable(Figure 3)Coronary angiogram done on day 4 confirmed findings on the Cardiac MRI and patient received angioplasty with a drug eluting balloon(Medtronic IN.PACT FALCON 2.5x20mm) delivered to the PLV branch(Figure 4).Patient was discharged well and he is scheduled for a staged PCI to the Left Circumflex Artery in the future.
   - Case Summary:
Right Ventricular Wall rupture is a rare and life-threatening mechanical complication associated with Myocardial Infarction. Clinical Suspicion followed by echocardiographic assessment can clinch the diagnosis early. Cardiac imaging plays an integral component in guiding therapy. Surgical intervention is the mainstay of treatment for a Right Ventricular wall rupture. This case exhibits a favourable prognosis owing to the nature of the myocardial wall tear which was subacute and self limiting. The formation of a mural thrombus at the rupture site limited the leakage. This together with timely revascularisation prevented a fatal condition, which is normally associated with high mortality.
|
|