Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191028_015
| ENDOVASCULAR - Aorta Disease and Intervention | |
| Thoracic Endovascular Aortic Repair: Emergent Consideration for Aortic Dissection Stanford Type B Treatment: A Better Outlook Compared to Medical Therapy Alone | |
| Farhanah Kamarudin1 | |
| Universiti Kebangsaan Malaysia Medical Centre, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
C.H.M
-Relevant clinical history and physical exam:
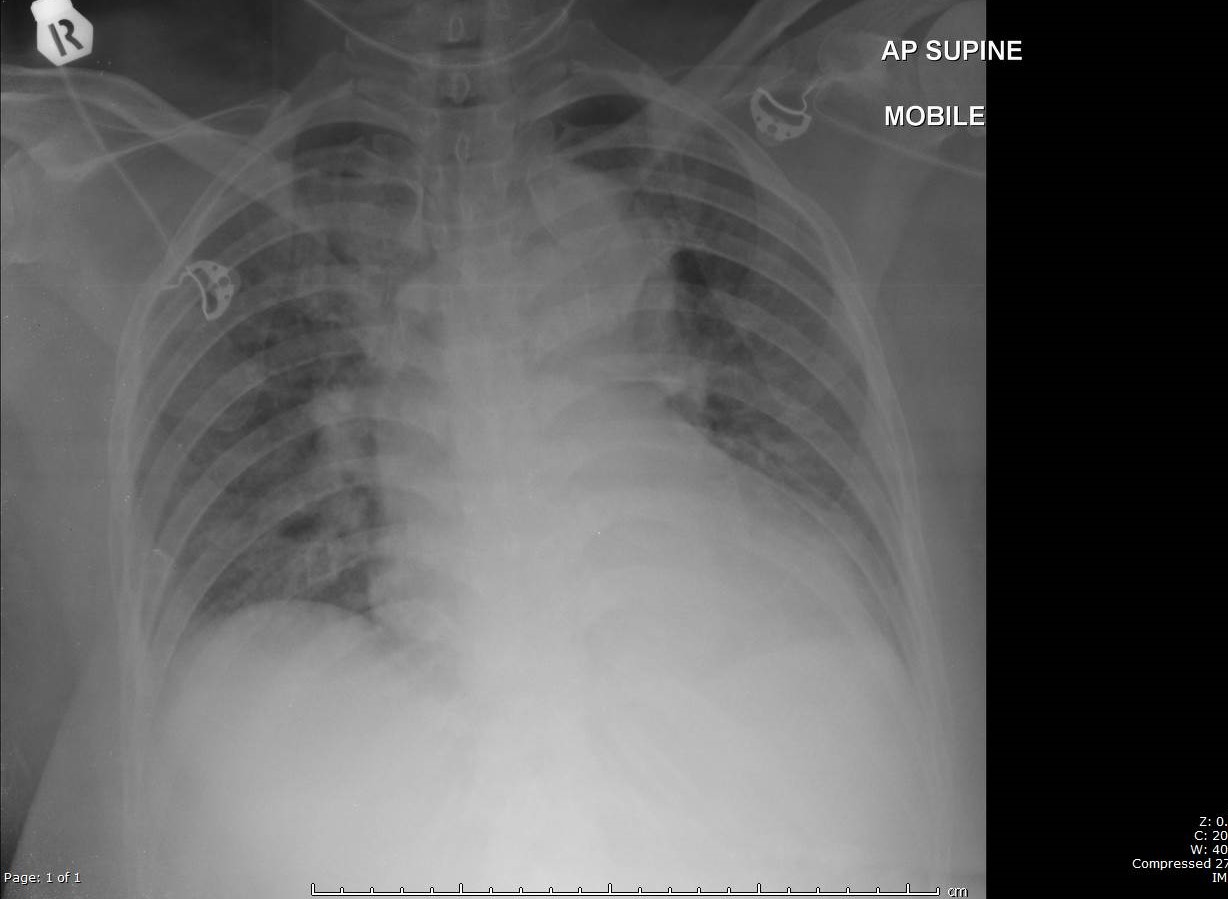
49 years old lady with underlying hypertension on 2 anti-hypertensive medication. Presented withabdominal pain for 2 months worsening in nature. Blood pressure was 170/98 mmHg& heart rate 86 bpm. Abdomen soft, non-tender & no mass palpable. Lungsauscultation reduced air entry at left lower zone. Peripheral pulses were normal.Later blood pressure labile range 121 to 230 mmHg requiring IV infusionlabetalol & sodium nitroprusside. Abdominal pain symptoms still present occasionally
 -Relevant test results prior to catheterization:
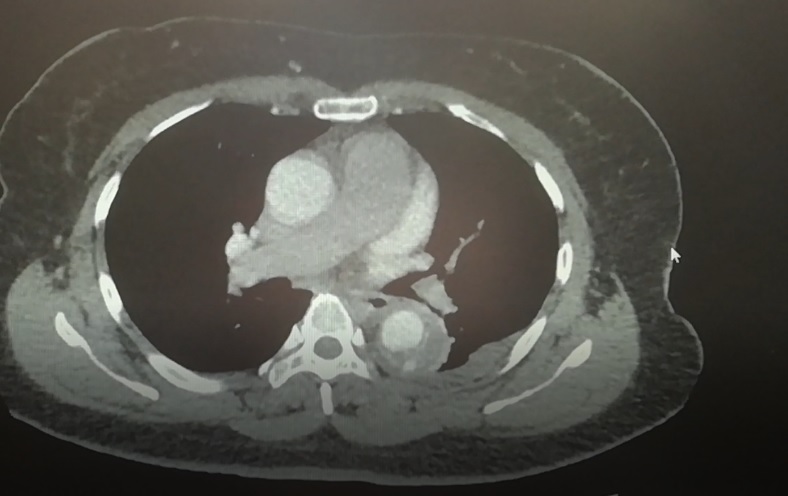
The repeat CT angiogram of chest and abdomen showed aortic dissection type B with intramural hematoma from distal part arch ofaorta to abdominal aorta at L1to L2level. Focal contrast was seen within the intramural hematoma at T8 level withmaximal thickness of the hematoma of 1.5 cm. There was also presence of left pleural effusionat the same time pointing towards leaking aortic dissection type B.
 - Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
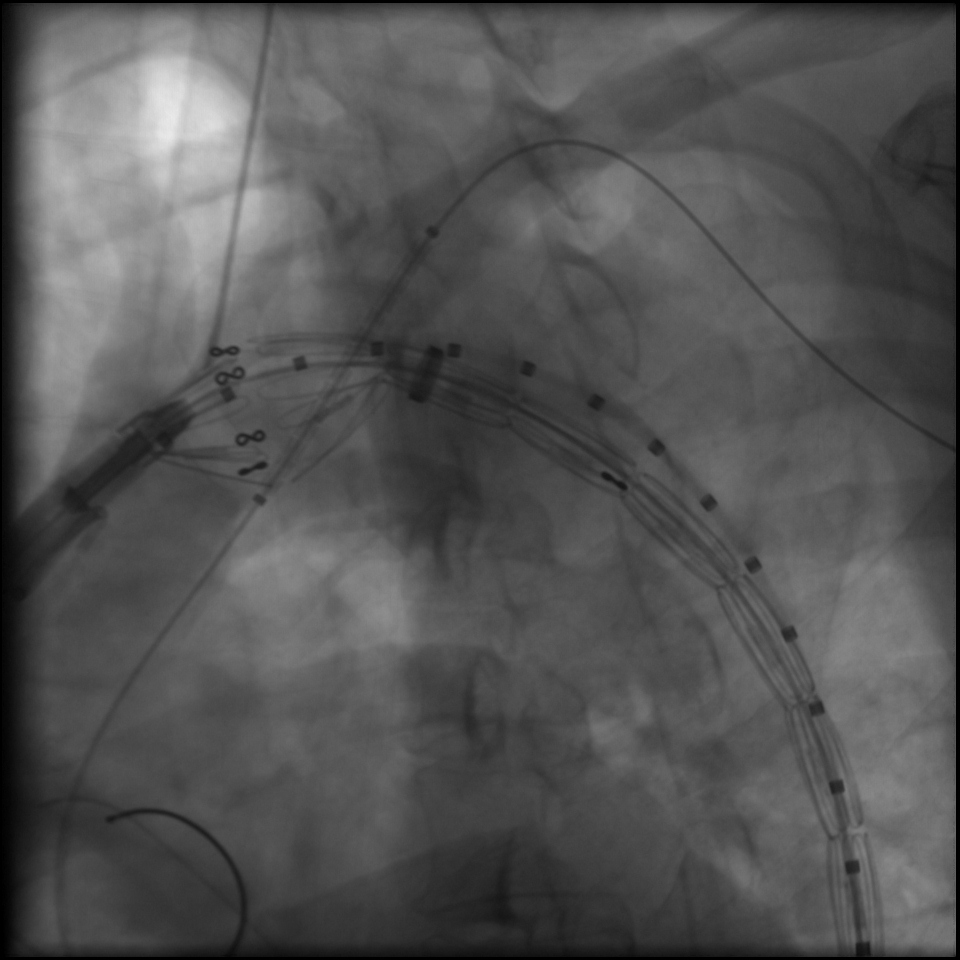
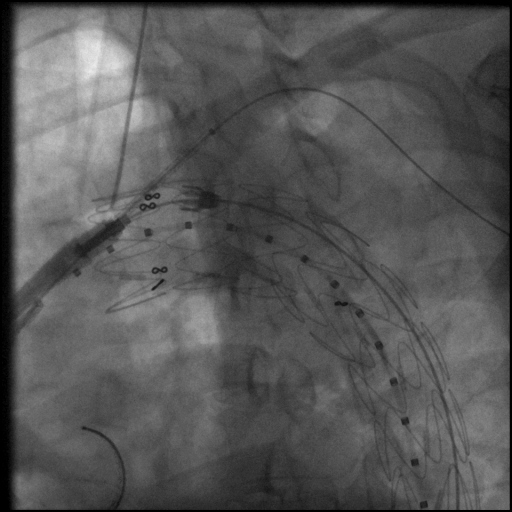
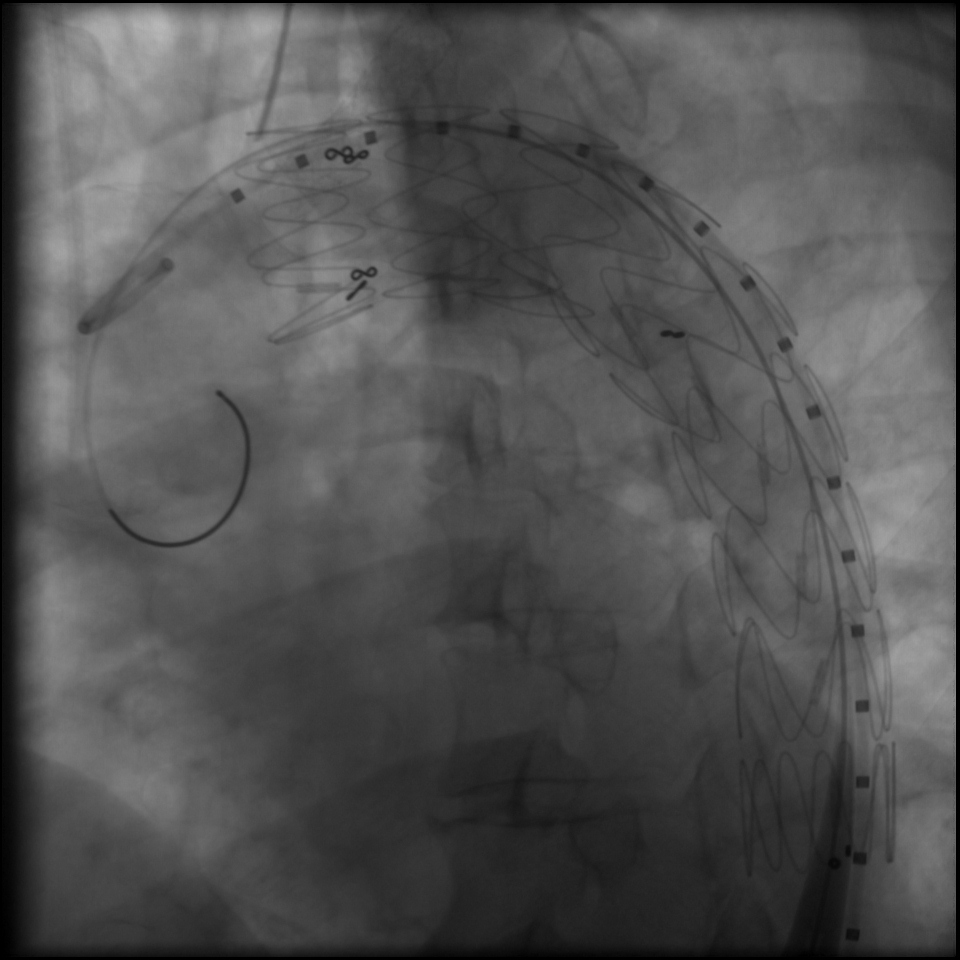
Thoracic Endovascular Repair with left Subclavian ArteryChimney under general anaesthesia for leaking aortic dissection type B. Spinal cord drainage was inserted by anesthetist to prevent paralysis complication.Both femoral arteries and leftbrachial artery were punctured to pass through a stent { Medtronic Valiant }size 28 mm x 150 mm intothe descending aorta. The stent was placed between subclavian arterybranch level of aortic arch and T7level of descending aorta. Then, another stent{ Advanta V12} size 8 mm x 38 mm was placed at the left subclavian artery as SubclavianArtery Chimney. Subclavian Artery Chimney applied was to ensurethe patency of left subclavian artery and at the same time guaranteed effectivesealing of the endograft stent to prevent future endoleak. The tear entry pointwas less than 2 cm from the subclavian artery and without another stent actingas the ‘chimney’, the endograft stent might not be able to provide good sealingcoverage. Once the stents were safely landed at the desired level, anesthetist helped to adjust blood pressure at systolic 80 mmHg before the stents wereexpanded to prevent stent migration and safely secured in place. The guide wire was pulled out and the arterial puncture sites wereclosed with Proglide closure device {Abbott Vascular}. Spinal drainage after 48 hours post procedure.
   - Case Summary:
Intervention for aortic dissection type B is made feasible and safer with proper preparation hence good option to be considered in this era of endovascular intervention. Current practice of conservation and monitoring blood pressure in ''uncomplicated'' aortic dissection is like a time bomb as blood pressure is labile and as intramural hematoma and aotic wall diameter progressed over time hence leads to complication with higher morbidity and mortality. As technology and knowledge advanced, intervention for aortic dissection with endovascular approach need chance to be proved as mainstream treatment for aortic dissection type B
|
|