Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191028_007
| CORONARY - Chronic Total Occlusion | |
| Anomalous Origin of Right Coronary Artery: The Hidden CTO! | |
| khalid Tammam, Raouf Shaaban4 | |
| , Dar Al Fouad Hospitals, Egypt4, | |
|
[Clinical Information]
- Patient initials or identifier number:
Patient #1
-Relevant clinical history and physical exam:
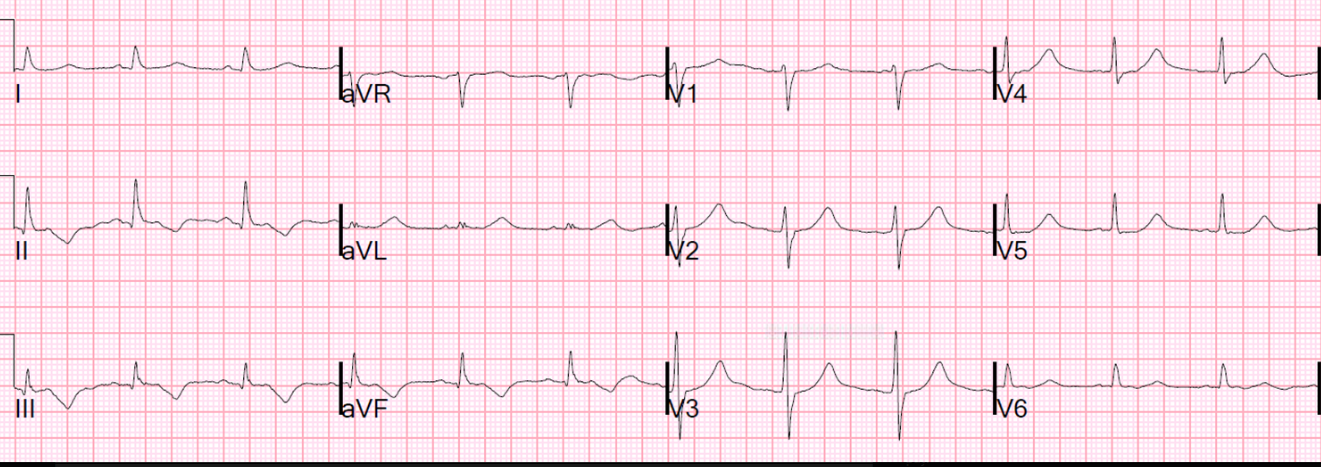
48 years old male, hypertensive,dyslipidemic and heavy smoker. He complained of exertional chest pain for 1 month duration, his ECG showed T wave inversion in inferior leads, transthoracic echocardiography showed hypokinesia in inferior and lateral walls. clinical examination showed equal air entry bilaterally, normal S1 and S2, peripheral pulsations felt well bilaterally. He was asked to do a MSCT coronaries.
-Relevant test results prior to catheterization:
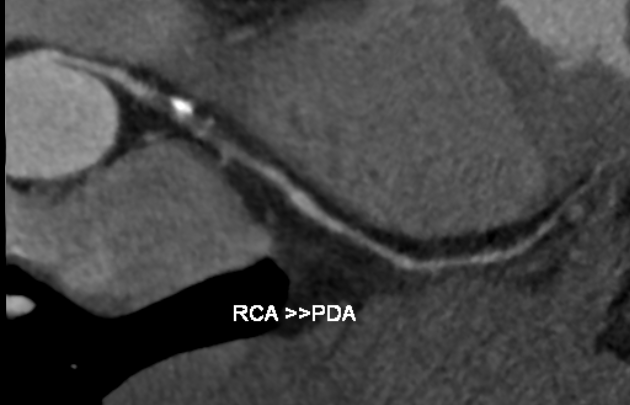
MSCT coronaries showed proximal total occlusion of calcified RCA and a non significant lesion in the mid-segment LAD.
   - Relevant catheterization findings:
Coronary angiography was done via the RT radial approach showing a non significant LAD lesion. Multiple trials were done trying to engage the RCA however; the artery couldn't be visualized at all. Many diagnostic catheters were used as: JR 3.5, Amplatz Left I, Amplatz Right II and multi-purpose catheter. A trace for the RCA could be visualized with a non selective injection, as the RCA appeared to be at a very high anomalous origin.
|
|
|
[Interventional Management]
- Procedural step:
The approach was shifted to the RT femoral, a guiding multipurpose catheter was used to selectively engaging the RCA after snaring the RCA using a 0.014 inches RUNTHROUGH floppy wire. Multiple projections confirmed totally occluded RCA at its proximal segment with retrograde filling from the LAD. A FINECROSS microcath. was introduced over the wire into the proximal RCA.An antegrade escalating wire technique was implemented to cross the CTO segment using: Fielder XT-R, PILOT 150, GAIA II and CONQUEST PRO 12. A RUNTRHOUGH intermediate wire was then introduced after confirming being in the true lumen from the retrograde injection. Predilatation was done multiple times using 1.5 x 20 mm and 2 x 15 mm balloons. PCI to mid-segment RCA was done using a 3.5 x 38 mm DES followed by a 3 x 18 mm overlapping DES. Postdilatation was done using a 3.5 x 15 mm NC balloon.
- Case Summary:
Anomalous origin of RCA is not a common scenario however; it added on to the difficulty of managing our case. Using all projection together with being guided with the MSCT coronaries made us able to imagine the position of the RCA. Snaring of the coronary artery before being selectively engaging is a remote option but it could be the only possible solution. It's a highly dependent step on the operator's experience and hand skills. Anomalous origin of a coronary artery together with a CTO is one of the most complex interventions yet proper planning and tools selection can guide to ultimate success.
|
|