Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191028_006
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| How Can a Proximal Optimization Technique Save an Important Hidden Side Branch in Case of Acute ST Elevation Myocardial Infarction? | |
| El Ghali Mohamed Benouna1 | |
| Ibn Rochd hospital, Morocco1, | |
|
[Clinical Information]
- Patient initials or identifier number:
B.O
-Relevant clinical history and physical exam:
60 years old male, heavy smoker and hypertensive under angiotensin II receptor antagonist. He was admitted to our department with complaint of typical chest pain. the clinical examination found a normal blood pressure and heart rate without any signs of heart failure or cardiac murmur.
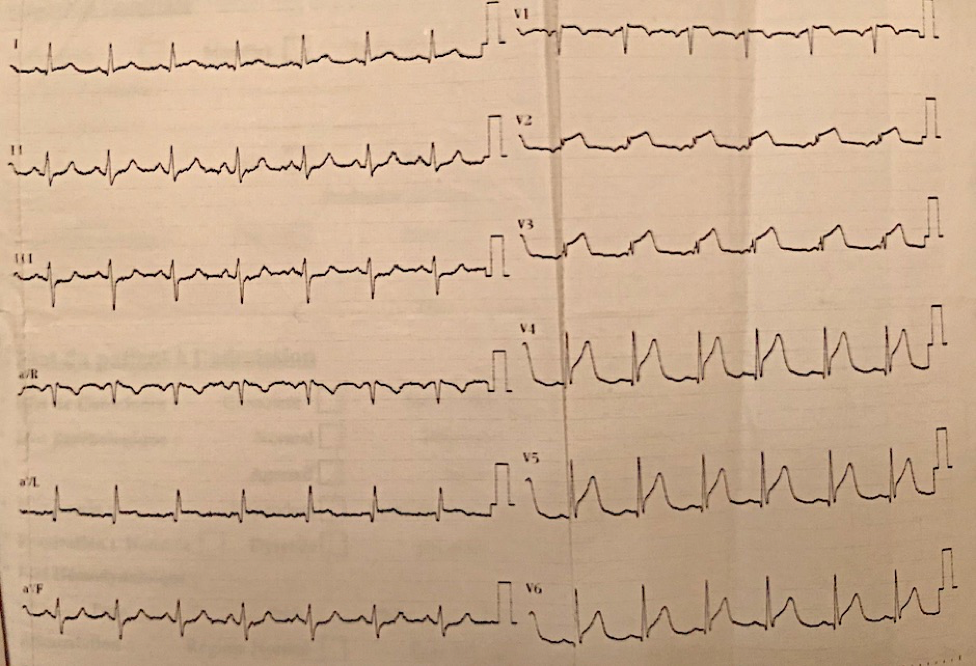
-Relevant test results prior to catheterization:
The electrocardiogram showed an ST elevation in anterior leads.
 - Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
An Extra Back Up 6 French guiding catheter intubate the left main. A balanced middle weight ( BMW ) wire cross the LAD occlusion without resistance, will be placed distally. A semi-compliant 2,5 X 15 mm balloon was inflated at 12 atmospheres front of the occlusion. The angiographic control showed a TIMI III flow in the LAD with severe and diffuse stenosis of the ostium of an important side branch. Another BMW wire failed to cross the ostium of this side branch related to a plaque shift wich leads to loose this important side branch. Because of the STEMI condition we decided to stent the first branch with 2,75 x 22 mm drug eluting stent, and performed a proximal optimization technique with a non compliant 3 X 15 mm balloon in order to open the stent struts front the ostium of the side branch. This manipulation allowed us to wire the important diagonal branch then we opened stent struts with 2,5 X 15 mm balloon to the side. A 3 X 22 mm drug eluting stent was placed into the side branch with a small protrusion in the LAD. A final kissing was performed with ana acceptable result.
- Case Summary:
The proximal optimization treatment is a mandatory step in bifurcation treatment even in the STEMI setting. In our case, this manipulation allowed us to bring back an important side branch. The chest pain disappeared and the echocardiography showed a 45 % ejection fraction. The patient was discharged three days later without any complication.
|
|