Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191028_004
| ENDOVASCULAR - Complications | |
| Salvage Endovascular Intervention for SVC Stent Failure | |
| Patrick Yan-Tyng Liu1, Jen-Kuang Lee1 | |
| National Taiwan University Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
JC Hsiao
-Relevant clinical history and physical exam:
This 62-year-old man presented to our hospital for progressive facial swelling in the past 1 month (Figure A). He also had arm swelling and dyspnea prior to this admission. SVC thrombosis was confirmed by CT scan, and he was found to have advanced lung cancer with multiple metastasis after further survey.
 -Relevant test results prior to catheterization:
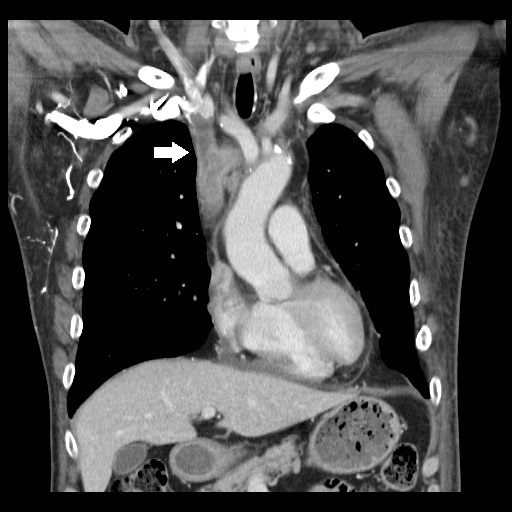
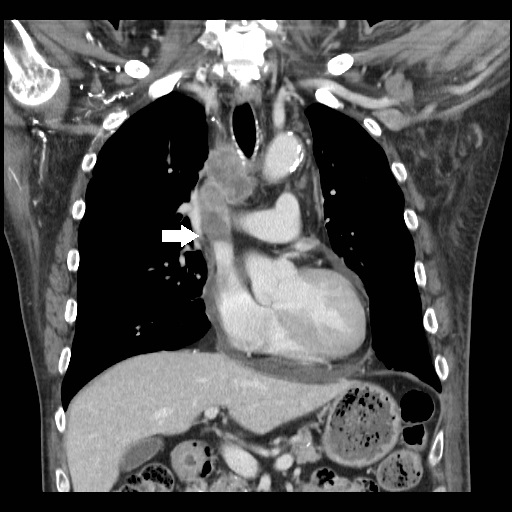
CT scan showed mediastinal lymph nodes with partial compression of bilateral brachiocephalic vein and SVC (Figure B). Filling defect was also noted at above sites in contrast-enhanced venous phase (Figure C, and D). According to both clinical history and image findings, SVC syndrome was diagnosed.
   - Relevant catheterization findings:
The patient received the first endovascular therapy (EVT) and total occlusion of right brachiocephalic vein was found (Video A). A 14 x 80mm Venono stent was placed from right brachiocephalic vein to SVC (Video B) after successful wiring and pre-dilatation. The patient did not get clinical improvement 5 days after the EVT, so we were consulted for the salvage procedure. In-stent thrombosis with total occlusion was confirmed by venography (Video C).
|
|
|
[Interventional Management]
- Procedural step:
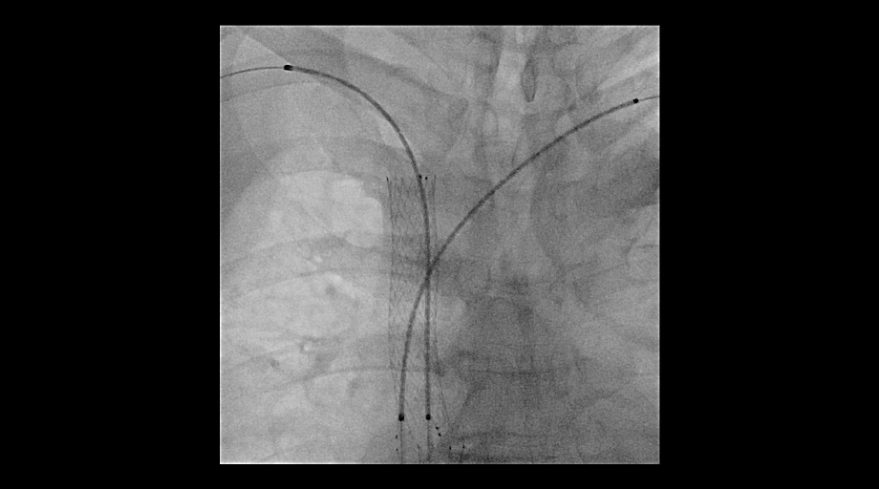
We retrogradely advanced 0.035” Terumo wire+ 4 Fr CXI microcatheter to right subclavian vein, and venography revealed the distal occlusion site. For left brachiocephalic vein, we performed antegrade venography and confirmed total occlusion at proximal brachiocephalic vein. To prevent thrombus dislodgement during further procedure, a SVC filter was implanted via right femoral approach. A 0.018” V-18 wire + 2.6 Fr CXI microcatheter was advanced to from left basilic vein, and penetrated into SVC stent with a 0.018" 300 cm Treasure 12 wire. Subsequently, wire was externalized (Rendezvous technique). After pre-dilatation, two 4 Fr Fountain infusion catheter was placed to bilateral brachiocephalic vein and urokinase catheter-directed thrombolysis (CDT) was performed (Video D).
 - Case Summary:
Comprehensive consideration and strategy for SVC syndrome stenting is mandatory. Inappropriate SVC stenting may not be helpful, but lead to catastrophic results. The followings are tips for a successful endovascular intervention of SVC syndrome. First, the obstruction level should be identified clearly with complete venography injected from right and left subclavian vein. Second, SVC filter is highly recommended to prevent possible thrombus dislodgement into pulmonary artery during the EVT procedure. Finally, stenting is necessary to reconstruct the vessel compressed by tumor. Simultaneous kissing strategy is most useful if SVC bifurcation is involved.
|
|