Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191027_011
| CORONARY - Adjunctive Procedures (thrombectomy, atherectomy, special balloons) | |
| Successful Rotational Atherectomy for the True Bifurcation Lesion in LMCA After CABG | |
| Nobuaki Igarashi1 | |
| Japanese Red Cross Kobe Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
2000594073
-Relevant clinical history and physical exam:
A-63-year-old female had taken a chest painat rest. She was taken to our hospital because of ACS. Emergency CAG revealed three vessel disease with severe calcification. While performing CAG, she had the VF which could be treated with electrical cardioversion. Because of high risk case, she underwent a coronary artery bypass graft (CABG). However, she was taken to our hospital again after 10 months. Emergency CAG revealed the stenosis at the anastomosis of the bypass graft.
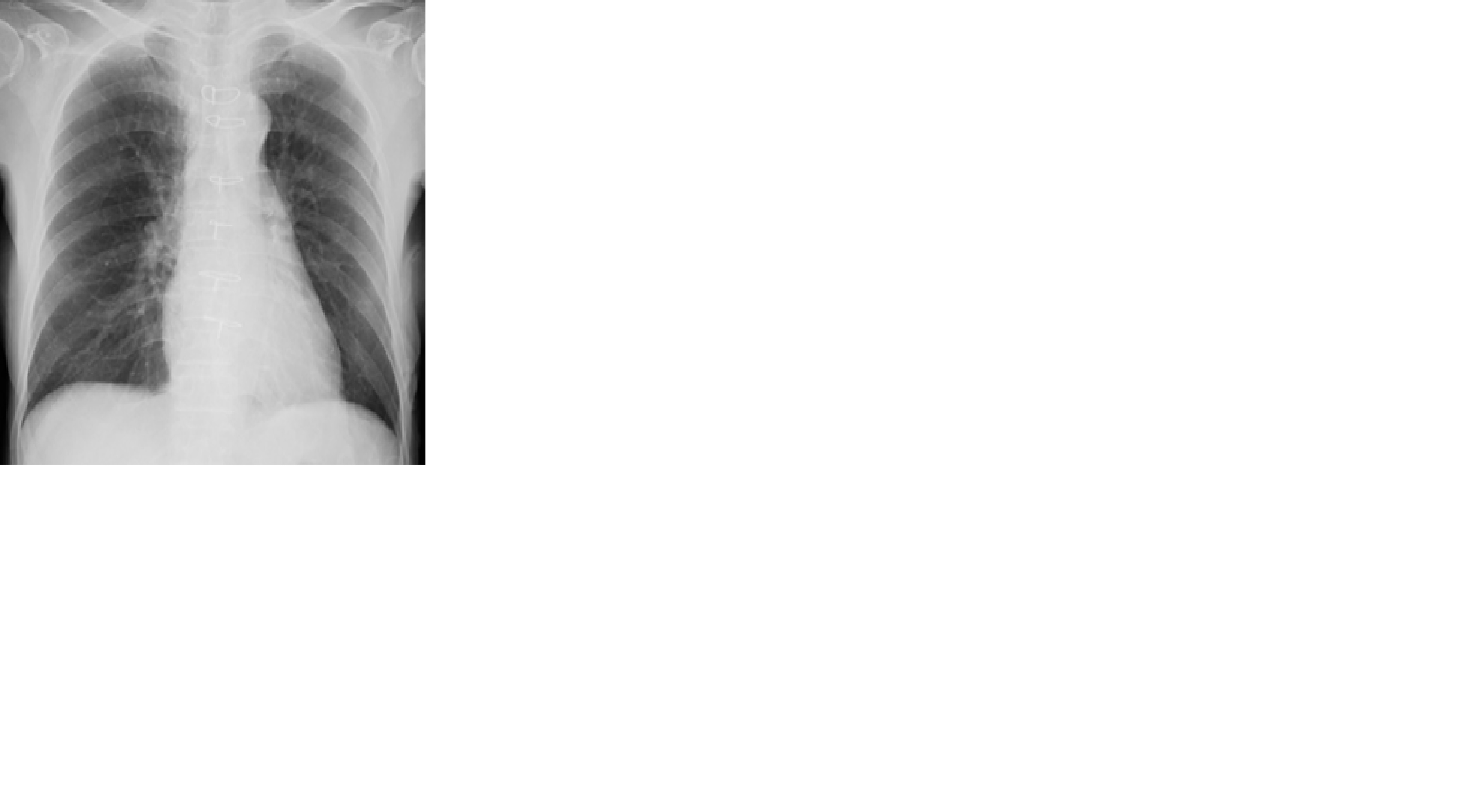
-Relevant test results prior to catheterization:
CTR was 49% in X-ray. ECG showed STelevation at aVR lead and ST depression at another lead. After disappearing of her symptom, ST-T change in ECG recovered. There was no asynergy in UCG. Ejecction fraction was 59%. Laboratory findings as follows:WBC 8100μL, Troponin T 0.01ng/ml, CPK165 IU/L, CKMB 17 IU/L,Cr 0.67mg/dl. eGFR 67.7ml/min/1.73m2 The coronary CT showed the severe caicified lesion at LMCA, LAD and LCx.
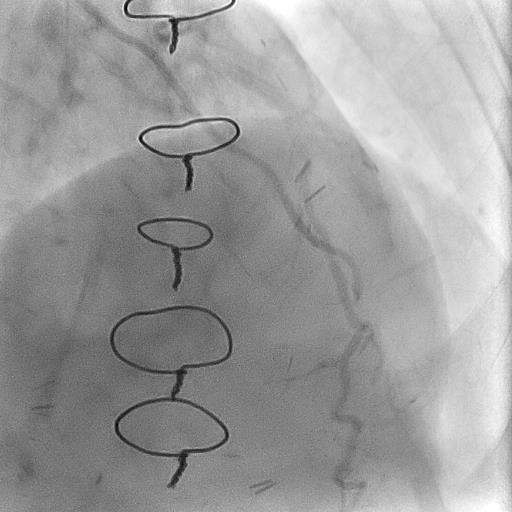
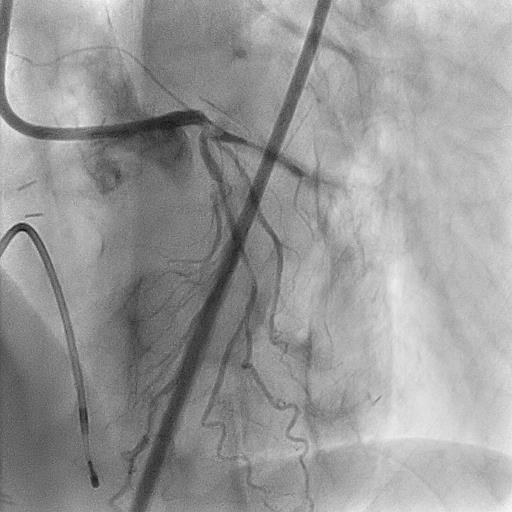
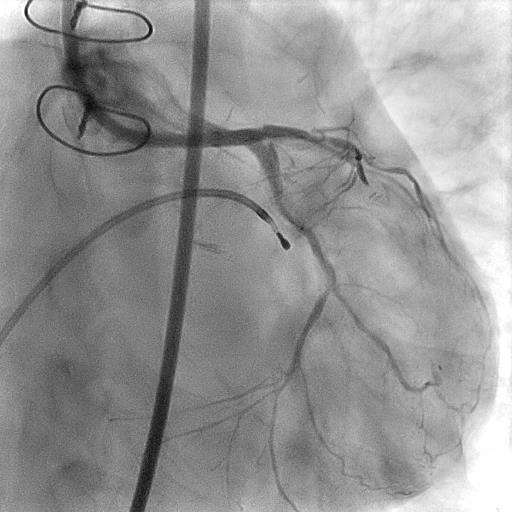
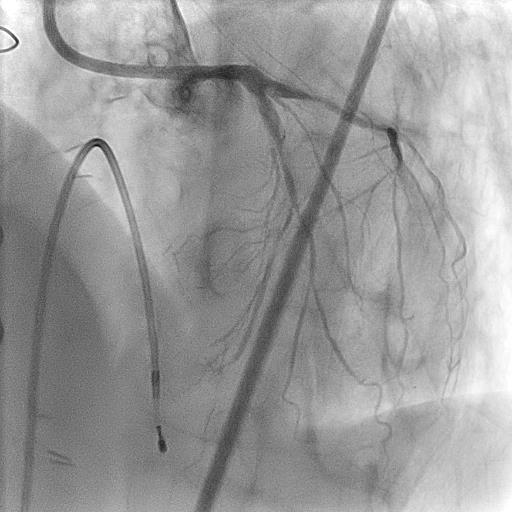
   - Relevant catheterization findings:
A coronary angiogram (CAG) showed stenosis at the anastomosis between right internal thoracic artery(RITA) and left anteriordiscending artery (LAD). Moreover, we saw stenosis at the anastomosis between leftinternal thoracic artery(LITA) and left circumflex (LCx). CAG and coronary CT revealed severe calcified lesion at Left main coronary artery (LMCA), LAD and LCx.
   |
|
|
[Interventional Management]
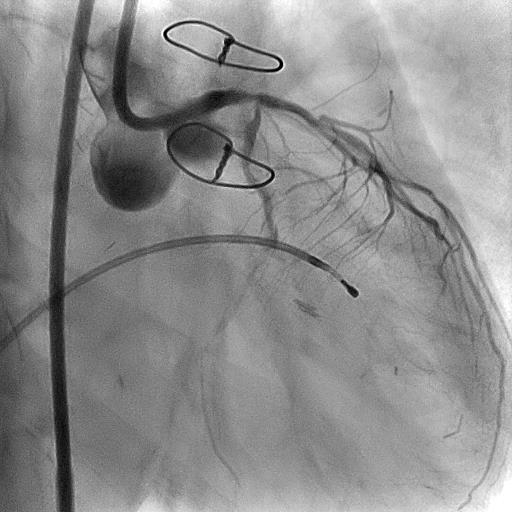
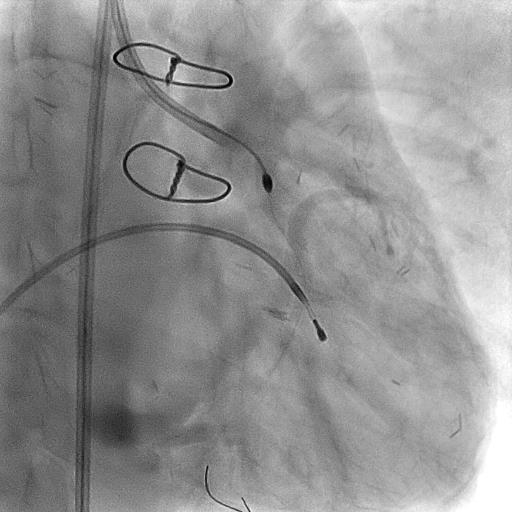
- Procedural step:
The conventional guidewire could advance into LAD and LCx. However, IVUS catheter didn’t cross into both branches. We changed the conventional guidewire with a RotaWire Extra support using microcatheter Caravel. The lesion from LMCA to LAD was ablated using 2.0mm burr with 200000rpm rotation at 10 times. Even if after this procedure, IVUS catheter didn’t cross to distal part of LAD. At that time, the calcification at carina sifted into the ostium of LCx site and then we saw the flow limitation at LCx.We advance the floppy type guidewire into LCx and then changed a RotaWire Extrasupport using microcatheter Caravel. The lesion from LMCA to LCx was ablated using 2.0mm burr with 200000rpm rotation at 5 times. After that, we saw a deepcut at opposite carina. To avoid coronary perforation, we didn’t treat here more this procedure. Because we thought 2.0mm burr was not enough from LMCA toLAD, Furthermore the lesion from LMCA to LAD was ablated using 2.25mm burr with 200000rpm rotation at 3times. After this procedure, IVUS findings showed calcification at the carina disappeared. We decided to separate this treatment into second attempt. Because we had to use more smaller size of 3rd Rota burr to ablate at distal part of LAD and there was tendency of slow flow. So we used 2.75mm cutting balloon from LMCA to LAD. Finally, we applied the drug at LMCA and LAD by using a DCB. At second attempt PCI, we performed Rotablar for distal part of LAD again with small size of burr.
   - Case Summary:
I successfully performed rotational atherectomy for true bifrucation lesion of LMCA after CABG. There was the calcified lesion at the carina. First ablation induced the carina shift of calcified lesion into LCx. Due to this phenomenon, moreover I could ablate the calcidfied lesion at the carina. Separated treatment might prevent from the no-reflow phenomenon.
|
|