Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191027_008
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| Bailout from the Balloon Catheter Stuck Due to the Un-Deflated Balloon During Endovascular Therapy for Iliac Artery | |
| Akinori Sumiyoshi1, Atsunori Okamura2, Mutsumi Iwamoto3, Satoshi Watanabe3, Hiroyuki Nagai4, Kota Tanaka3, Satoshi Suzuki3, Hirokazu Tanaka3, Kenshi Fujii3 | |
| Sakurabashi Watanabe Advanced Health care Hospital, Japan1, Sakurabashi Watanabe Advanced Healthcare Hospital, Japan2, Sakurabashi Watanabe Hospital, Japan3, Saint Joseph's Translational Research Institute, USA4, | |
|
[Clinical Information]
- Patient initials or identifier number:
M.T
-Relevant clinical history and physical exam:
A 70-years-old man with a history of hypertension and dyslipidemia was admitted to our hospital in April 2019. He has intermittent claudication of bilateral lower limbs within 300 meters, a Rutherford classification of grade I-2.He was given cilostazole(200mg) and clopidgrel(75mg).5. His resting ankle brachial index (ABI) score of his right leg was 0.87 and his left leg was 0.90.
-Relevant test results prior to catheterization:
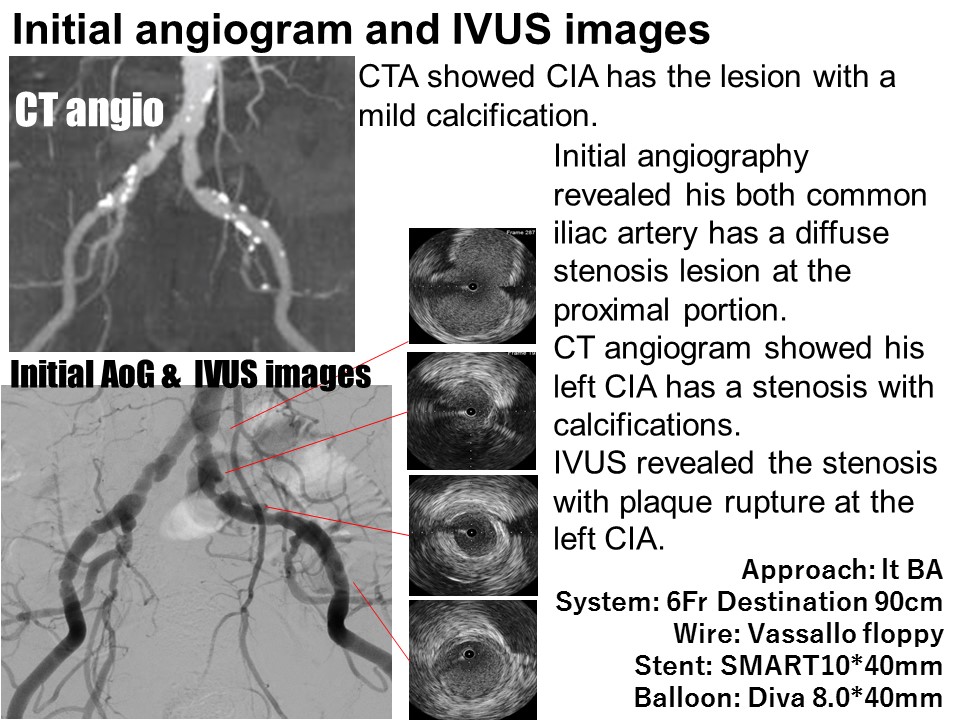
Echography revealed the both common iliac artery (CIA) has a stenosis lesion.CT angiogram showed CIA has the lesion with a mild calcification.
- Relevant catheterization findings:
Initial angiography revealed his both common iliac artery has a diffuse stenosis lesion at the proximal portion.
 |
|
|
[Interventional Management]
- Procedural step:
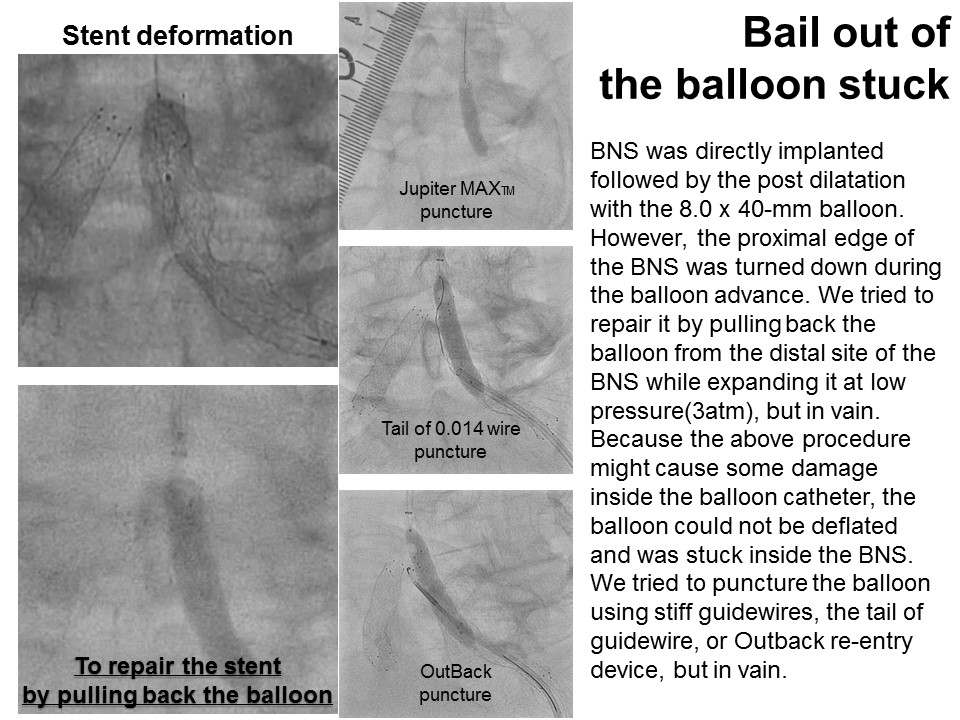
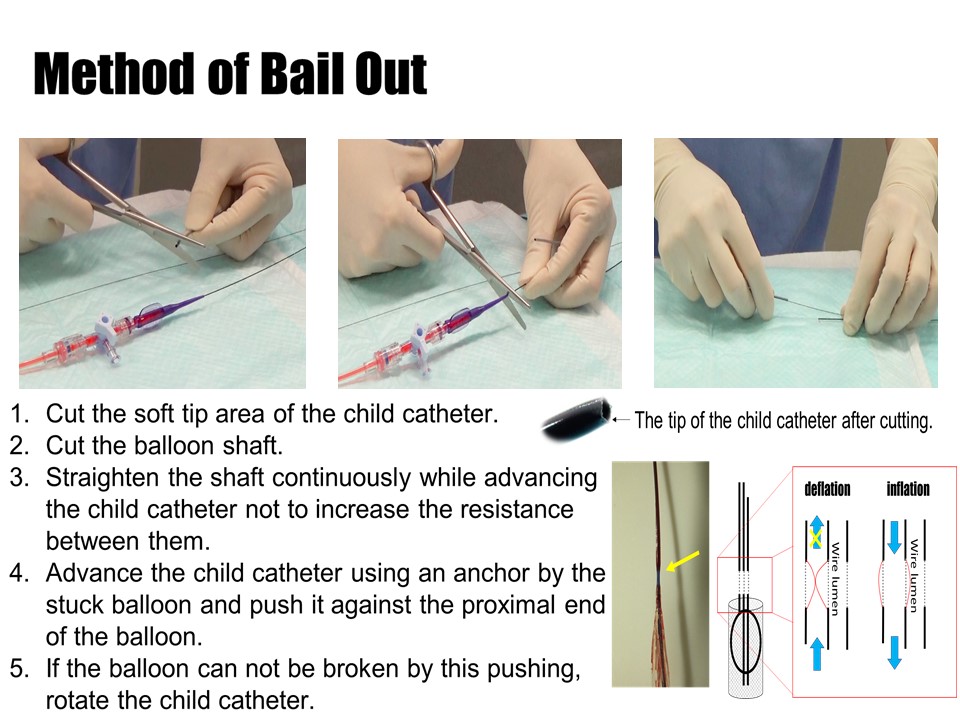
Firstly, the right CIA was dilated with an 8.0 x 40-mm balloon followed by implanting bare nitinol stent (BNS). We moved onto EVT for the left CIA. Because of the simple lesion, BNS was directly implanted followed by the post dilatation with the 8.0 x 40-mm balloon. However, the proximal edge of the BNS was turned down during the balloon advance. We tried to repair it by pulling back the balloon from the distal site of the BNS while expanding it at low pressure, but in vain. Because the above procedure might cause some damage inside the balloon catheter, the balloon could not be deflated and was stuck inside the BNS. We tried to puncture the balloon using stiff guidewires, the tail of guidewire, or Outback re-entry device, but in vain. Therefore, we used a 5-Fr child-catheter (ST01) whose tip was cut for the inner blades to be exposed. The ST01 was advanced and pushed strongly against the proximal end of the balloon by the balloon anchoring using the stuck balloon. The balloon was broken and deflated, which was confirmed by the leak flow of the contrast medium from the balloon. Post dilation was performed with the 8.0*40mm balloon.
  - Case Summary:
When the balloon can not be deflated, increase the negative pressure using a large syringe, or re- pressurize and slowly reduce the pressure.If it is difficult to deflate the balloon using the above methods, consider the balloon burst technique using the inner blades of the child catheter.
|
|