Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191027_004
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| A Lotus Root-Like Appearance in Coronary Arteries Visualized with Optical Coherence Tomography | |
| Shunpei Ushimaru1 | |
| Rakuwakai Otowa Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Case1: HO, Case2: HO
-Relevant clinical history and physical exam:
Case1: The patient was a 59-year-old male. He had a medical history of diabetes, hypertension, dyslipidemia and chronic kidney disease. He had been undergone maintenance hemodialysis for 3 years. Coronary artery bypass grafting (LITA-LAD) was performed a year ago.
-Relevant test results prior to catheterization:
Case1: Transthoracic echocardiography showed asynergy in anterior and inferolateral wall. Myocardial stress perfusion scintigraphy revealed myocardial infarction with ischemia in inferolateral wall area.Case2: She was diagnosed with old myocardial infarction, that was based on QS pattern and poor R wave progression in leads V1, V2, V3 and V4, and adenosine myocardial stress perfusion scintigraphy resulted in myocardial infarction with ischemia in anteroseptal wall area.
- Relevant catheterization findings:
Case1: A coronary bypass graft was patent. Coronary angiography revealed hazy and slit lesions in left circumflex (LCx) and right coronary artery (RCA).Case2: We observed a slit lesion in the mid portion of LAD. RCA and LCx were intact.
   |
|
|
[Interventional Management]
- Procedural step:
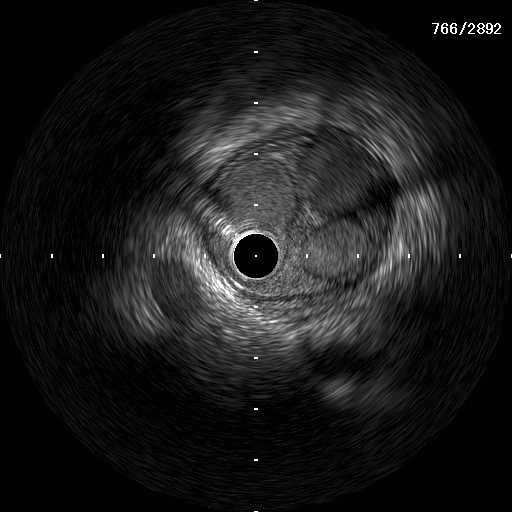
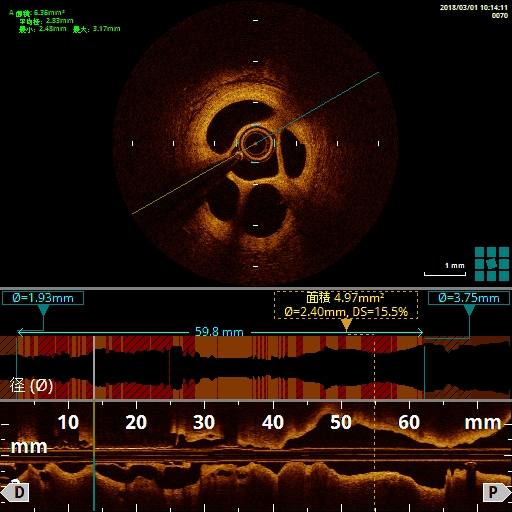
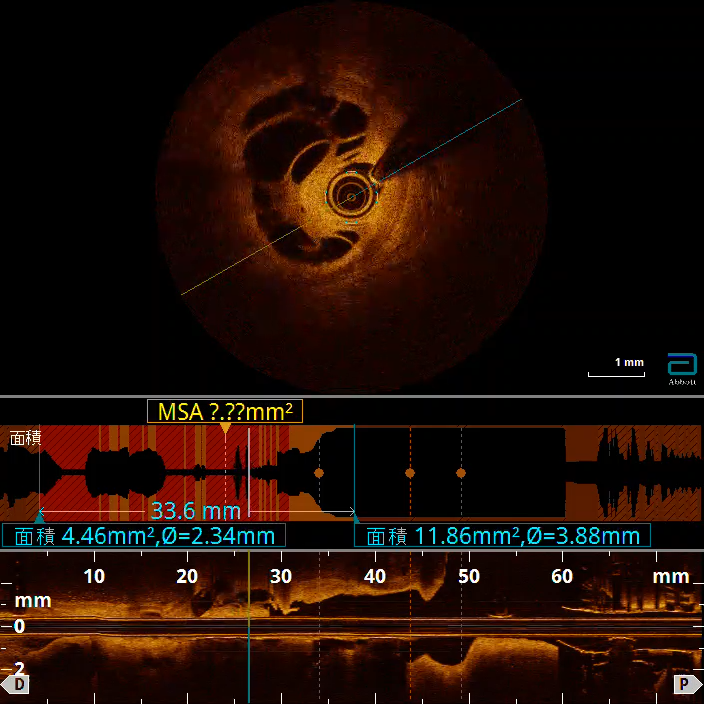
Case1: We planned PCI to LCx that myocardial perfusion areas were larger than RCA. The lesion was crossed with a 0.014-inch guidewire. A 60MHz IVUS catheter was advanced into obtuse marginal branch of LCx to investigate intravascular constitution. The IVUS showed a lotus root-like appearance with multiple intraluminal channels of various sizes. Subsequently, we used optical coherence tomography (OCT) to verify which lumen side branches divaricated from. We confirmed that side branches were branched off from the lumen that a guidewire crossed. Predilatation was performed with a semi-compliant balloon, then a drug eluting stent was deployed. PCI was successful without occlusion of side branches.
   - Case Summary:
We experienced 2 cases of lotus root-like appearance in multiple coronary arteries. In first case, OCT guided us that which lumen divided into side branches in the multiple channels. That helped which lumen we should dilate and deploy a stent in. Next case, IVUS images showed less information, but OCT gave clearer images of a lotus root appearance because of its high spatial resolution.
|
|