Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191026_001
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| Endovascular Treatment for Buerger‘s Disease with Long-Term Clinical Course | |
| Taku Kato1 | |
| Rakuwakai Otowa Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
HK
-Relevant clinical history and physical exam:
The patient was a 76 years old male who had a had a history of Buerger’s disease for about 40 years.
   -Relevant test results prior to catheterization:
The ABI and SPP values were extremely low in both feet, especially in the right side.
   - Relevant catheterization findings:
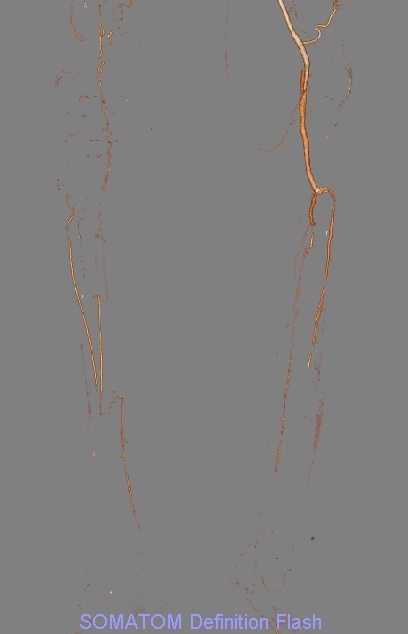
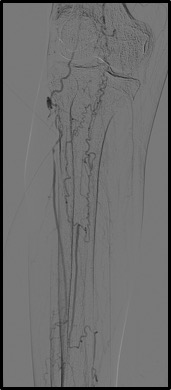
I planned two phased treatment meaning that I treat the right iliac artery and the left SFA from right groin approach in first session, and next treat the infrainguinal lesions in the right side in second session.
 |
|
|
[Interventional Management]
- Procedural step:
In first session, I implanted a self-expandable stent in the right iliac artery, and, next treated the chronic total occlusion (CTO) of the left SFA. In the CTO lesion, I advanced the 0.014-inch guidewire intraluminaly with IVUS guidance. I dilated two DCB catheters after successful guidewire crossing, and final angiography showed favorable flow in the left SFA.
- Case Summary:
Because many lesions of Buerger’s disease are inappropriate for stenting and shrinkage vessels, intraluminal wiring using IVUS may be important and useful.
|
|