Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191025_005
| CORONARY - Chronic Total Occlusion | |
| If You Keep Knocking, You Will Find Open Door. | |
| Afrah Yousif Haroon1 | |
| National Heart Institute, Malaysia1, | |
|
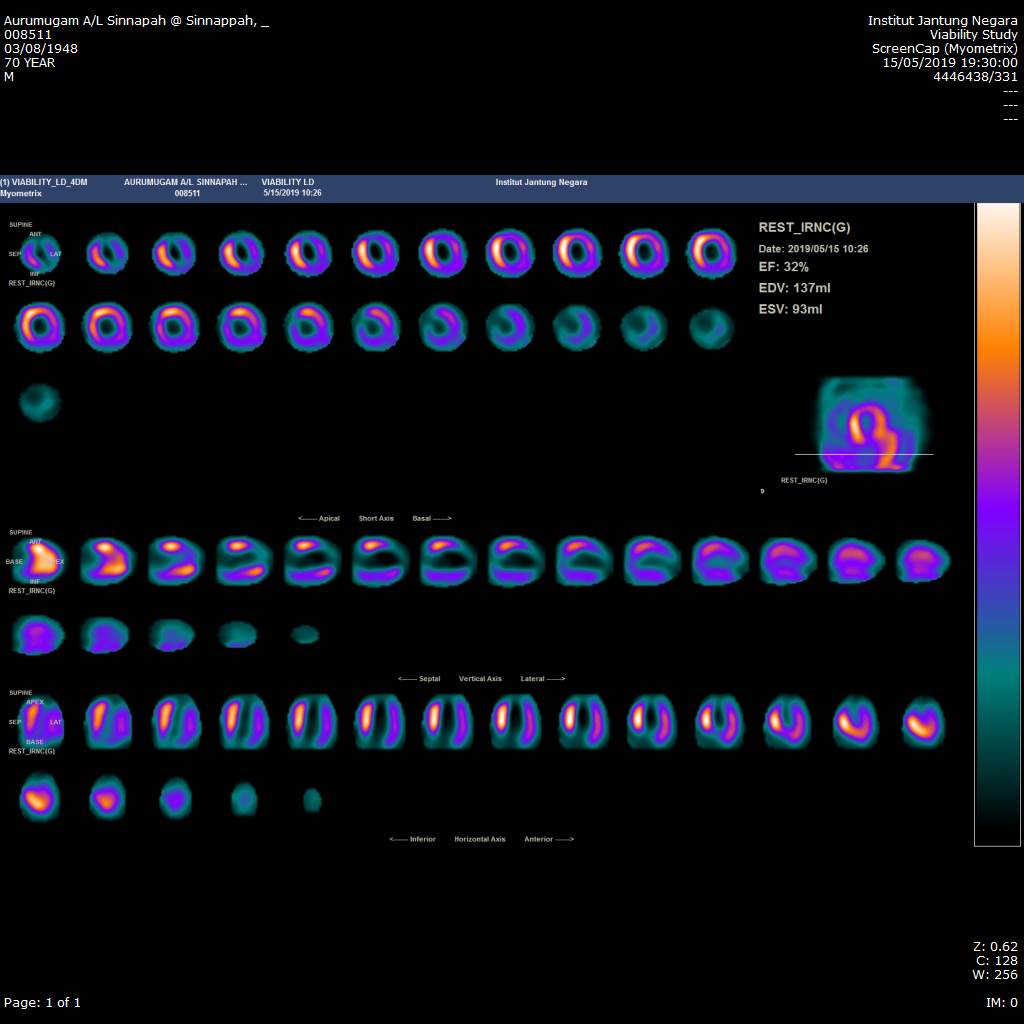
[Clinical Information]
- Patient initials or identifier number:
ASS
-Relevant clinical history and physical exam:
A 71 years male, has recent anterior MI, successfully thrombolysedwith Metalyse. April 2019.
-Relevant test results prior to catheterization:
Blood test : Troponin -T 1320Renal profile & full blood count were normal.angiogram: severe TVD CTO LAD, CTO RCA, Stumps all SVG: since 2016
 - Relevant catheterization findings:
Double puncture, RRA 7F sheath & RFA 7F sheath.
|
|
|
[Interventional Management]
- Procedural step:
IVUS guided fielder XT wire in Corsair MC
Guidezela used to deliver synergy stent 2.5/48 to d-mLAD - Case Summary:
Learning points
|
|