Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191023_003
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Shortened Provisional Stenting with Distal Final Kissing: A Modified Provisional Stenting Technique for Some True Coronary Bifurcation Lesions | |
| Mutlu Vural1 | |
| Private clinic, Turkey1, | |
|
[Clinical Information]
- Patient initials or identifier number:
AA
-Relevant clinical history and physical exam:
-Relevant test results prior to catheterization:
The ECG showed previous anterior MI.Anterior and apical hipokinesia with 50% ejection fraction were also shown byECHO.
 - Relevant catheterization findings:
On coronary angiography, right coronaryartery was normal (video 1). On the other side, a diffuse LAD instentrestenosis (probably stent undersized) with moderate left main distal eccentricstenosis were demonstrated (Video 2a and 2b). Distal bifurcation lesion after LAD instent restenosis was a true bifurcation lesion(BL) with small sized side branch (SB) and distal main vessel (MV), both wereless than 2 mm.
 |
|
|
[Interventional Management]
- Procedural step:
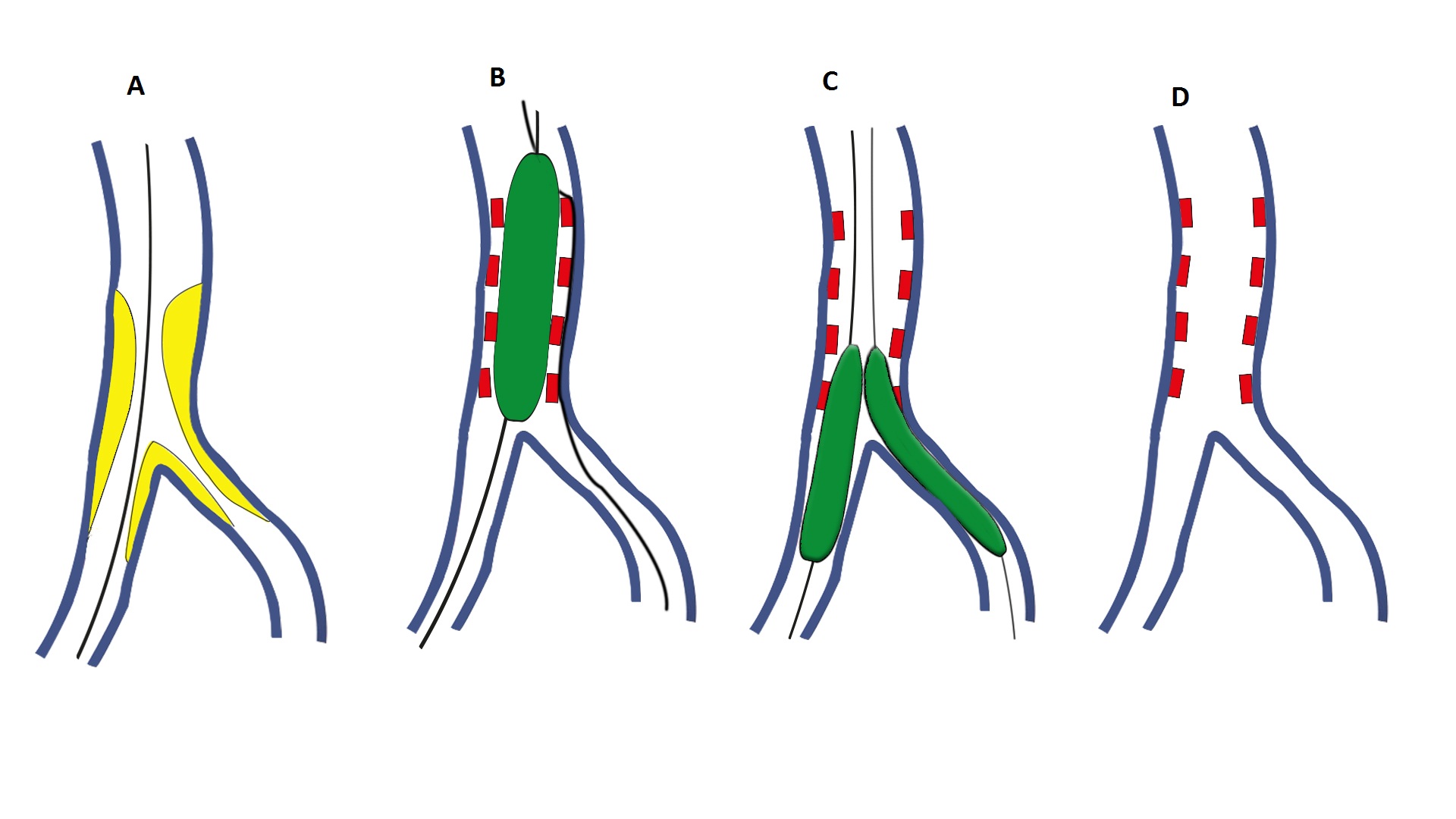
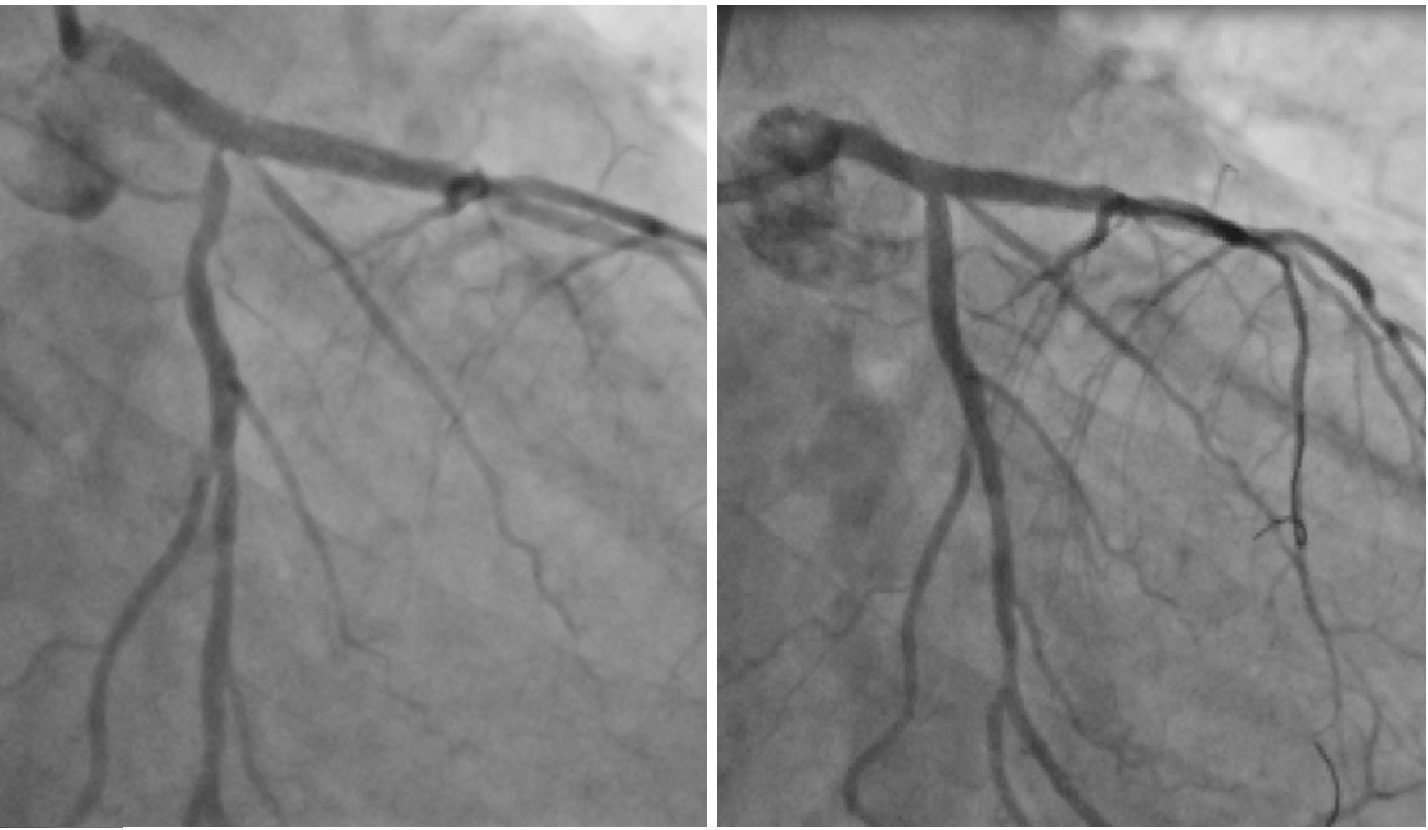
There has been severe instent restenosis in the proximal LAD in which the ostium was not fully covered by the previous stent. Both distal MV and major SB of the LAD had also critical but limited disease (<10 mm). After ballon angioplasty, LM to LAD crossover drug-eluting stent implantation (circumflex ostium was clear) just before the distal bifurcation (Video 3) has been followed with distal final kissing with two 2.0 mm balloons (Video 4). Final result was satisfactory except a minor dissection in the SB (Video 5). Illustration of the technique shows the procedure step by step (Figure 1). It is called shortened provisional stenting (covering only proximal MV) with distal final kissing which would be successfully performed in some cases with true BL, especially when both DMV and SB diameters are small in diameter and have limited disease. Unfortunately, 2 mm drug coated balloon was not available in our cath lab. Nevertheles, control angiography (11 months later) confirmed long-term patency of this technique and healing of the dissection (Video 6). We failed in the LM-to-LAD crossover stenting with LCX osteal stenosis 11 months later (Figure 2A). Late reverse crush technique was performed and ended with final kissing and optimal final result (video 7, Figure2B and video 8).
- Case Summary:
The superiority of "single-stent technique" and "two-stent techniques" in true BLs is a never-ending discussion between interventional cardiologists. In most bifurcations with a significant stenosis in both branches, a provisional strategy of stenting the main branch only is effective, with theneed to implant a second stent on the side branch occurring in approximately one third of cases. Shortened provisional stenting with distal final kissing would be successfully performed in some cases with true BL, especially when both distal MV and SB are small in diameter and have limited disease (<10 mm).
|
|