Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191022_001
| CORONARY - Chronic Total Occlusion | |
| Double CTO of LAD with Complex Anatomy Both Retrograde and Antegrade Approach | |
| Raghav Sharma1, Arvind Yuvaraj Narasimhan2, N Prathap Kumar3 | |
| RKM Hospital, India1, Sri Narayani Hospital and Research Center, India2, Meditrina Hospital, India3, | |
|
[Clinical Information]
- Patient initials or identifier number:
S
-Relevant clinical history and physical exam:
48 M, presented with angina on exertion NYHA functional class III symptomsPast h/o: no h/o DM, HTN ++, h/o PTCA to RCA done in some hospital with CTO ofLAD and ? attempted PTCA to LADsurgeon opinion sought; poor targets for CABGPersonal h/o: smoker++, alcholic++, no significant family h/oClinical examination: BP 150/90 mmHg PR: 80/min, CVS and RS : normal
-Relevant test results prior to catheterization:
Labs : All labs including viral markers were normalECG: NSR with no significant ST-T waves changesEcho: No RWMA LVEF 50% with no valvular leaks
- Relevant catheterization findings:
Distal LM tapering lesion involving ostium of LAD and LCXLAD: Ambiguous origin occluded 100% at the level of diagonalLCX: Diffuse disease involving both om which is significantRCA: Stent seen in mid RCA wih 70% lesion proximal to stent and tandom 90% lesion distal to stentMid and distal LAD seen filling from collateral from RV branch and distal LAD diffuse disease with CTO after collateral from RV branch
|
|
|
[Interventional Management]
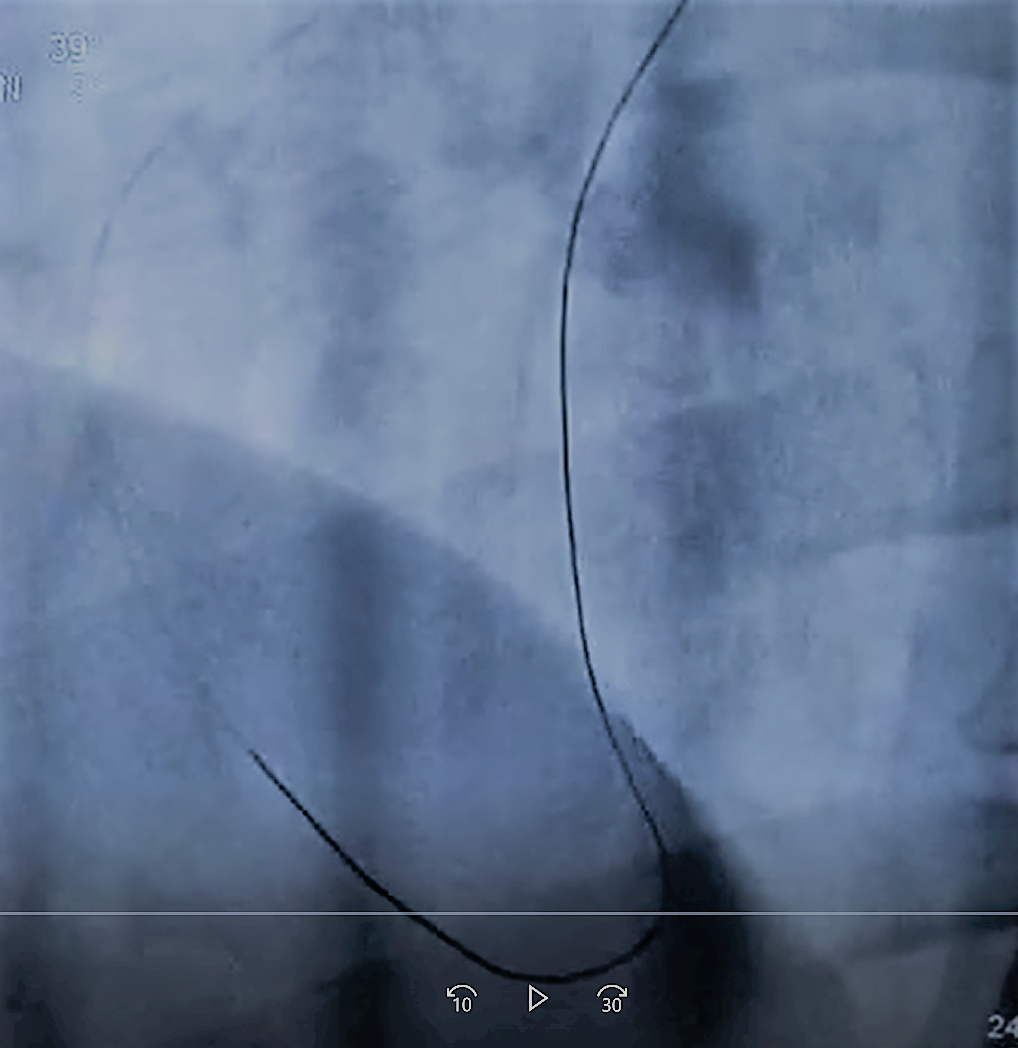
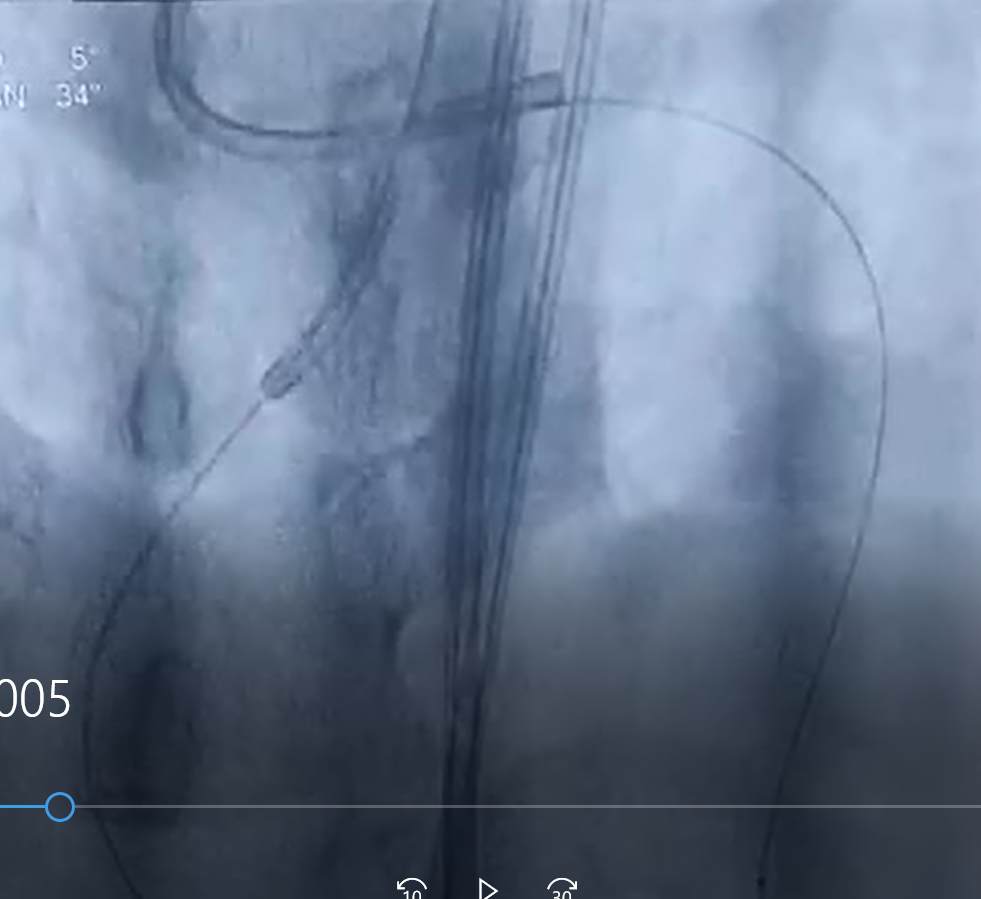
- Procedural step:
7F JR was taken and RCA was engaged simultaneously 7F XB was taken & LM was engaged. Fielder XT R was taken crossed via struts of RCA stent into RV branch, after identifying collateral it was parked in LAD retrogradely. Fine cross was taken over Fielder XT R & was parked in LAD, Fielder XT R was exchanged with Gaya II wire and lesion was crossed retrogradely via Gaya II it was parked into XB. 2.75x10 balloon was taken in XB antegradely & inflated at 10 ATM pressure to anchor Gaya II and fine cross was parked in XB. Fielder FC exchange length wire was taken & snared out through XB over Fielder FC 1.5x10 CTO balloon was taken & lesion was dilated till mid LAD. Diffuse dissection of LAD was noted, another fielder FC was taken parallel to exchange length Fielder FC antegradely to cross another CTO after mid LAD but failed. Fine cross was parked retrogradely into XB & another fine cross was taken antegradely & both fine cross were kissing mouth to mouth. Fielder XT R was crossed through both and parked into mid LAD. Fine cross was taken antegradely wire was exchanged with fielder FC & with support of fine cross wire could cross second CTO antegradely & parked in distal LAD lesion was dilated with 1.5x10 CTO balloon and 2.5x10 compliant balloon two stents 3x40 mm & 2.75x40mm DES was deployed from distal LM to distal LAD at 15 ATM pressure & was post dilated with 4x10, 3x10 NC balloon TIMI grade III flow seen.
   - Case Summary:
Here we present acase of double CTO with both antegrade and retrograde approach denied for CABG due to poor targets correct material usage, identifying correct collateral, presence of mind and good concepts plus proper training plays a crucial role in attempting as well as opening complex arteries. Idea of presenting this case is that it is not only complex but technically also challenging.
|
|