Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191021_009
| CORONARY - Chronic Total Occlusion | |
| Rescue of a False Lumen Stent Implanted in Right Coronary Artery Chronic Total Occlusion | |
| Heng Shee Kim1, Chu Zhen Quek1, Gurudevan Mahadevan1, Chuey Yan Lee2, Hou Tee Lu1 | |
| Sultanah Aminah Hospital, Malaysia1, Hospital Sultanah Aminah, Malaysia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
SBS
-Relevant clinical history and physical exam:
A 53-year-old male, smoker, with underlying hypertension admitted to a private hospital for acute coronary syndrome, and subsequently the patient was referred to our center for CABG because of failed percutaneous coronary intervention (PCI). On arrival, he had NYHA I, CCS I – II symptom.
-Relevant test results prior to catheterization:
ECG: sinus rhythm with Q wave inferior lead
- Relevant catheterization findings:
CAG at previous centerLM 50%pLAD 95%mLAD 60%pLCx and dLCx 50%pRCA 50%, CTO mRCAdistal RCA stent implanted into false lumen causing no re-flow from mRCA onwards
Repeated CAG in our center: similar finding with total occluded mRCAReferred for CABG, patient declined. We performed an IVUS guided PCI to:pLAD and mLAD with Resolute Integrity 3.0x34pLCX with Impact Falcon 3.0x20ostial LM to ostial LAD with Resolute Integrity 4.0x12 Planned for staged PCI to CTO mRCA in 1 month. 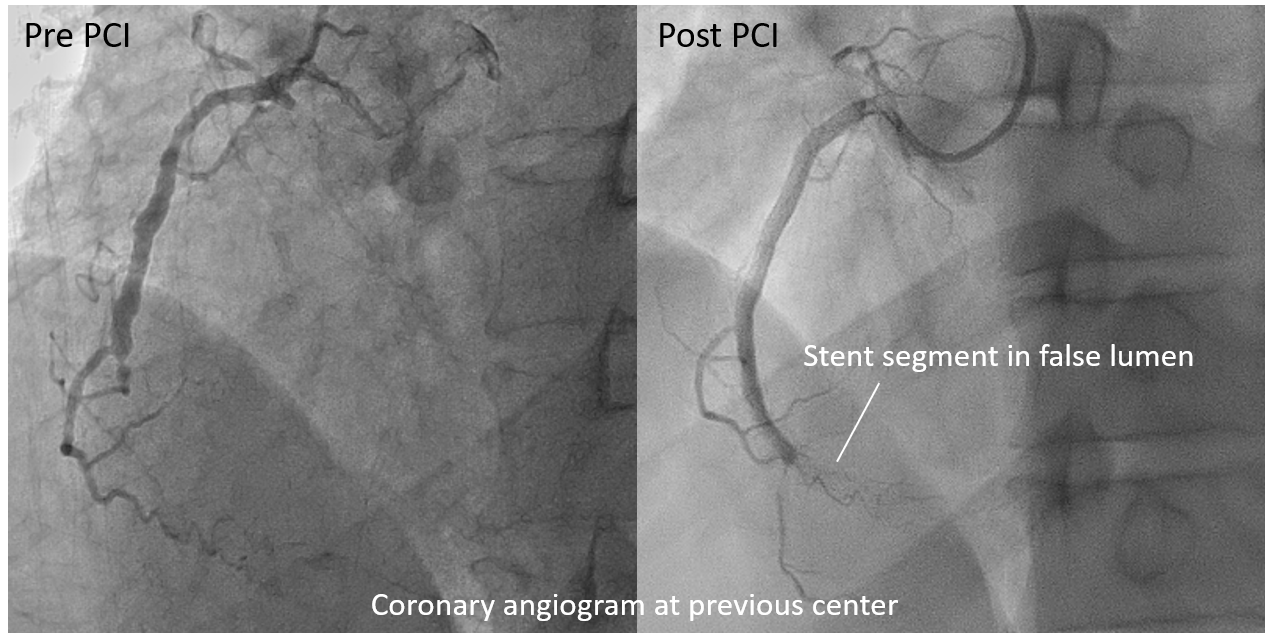 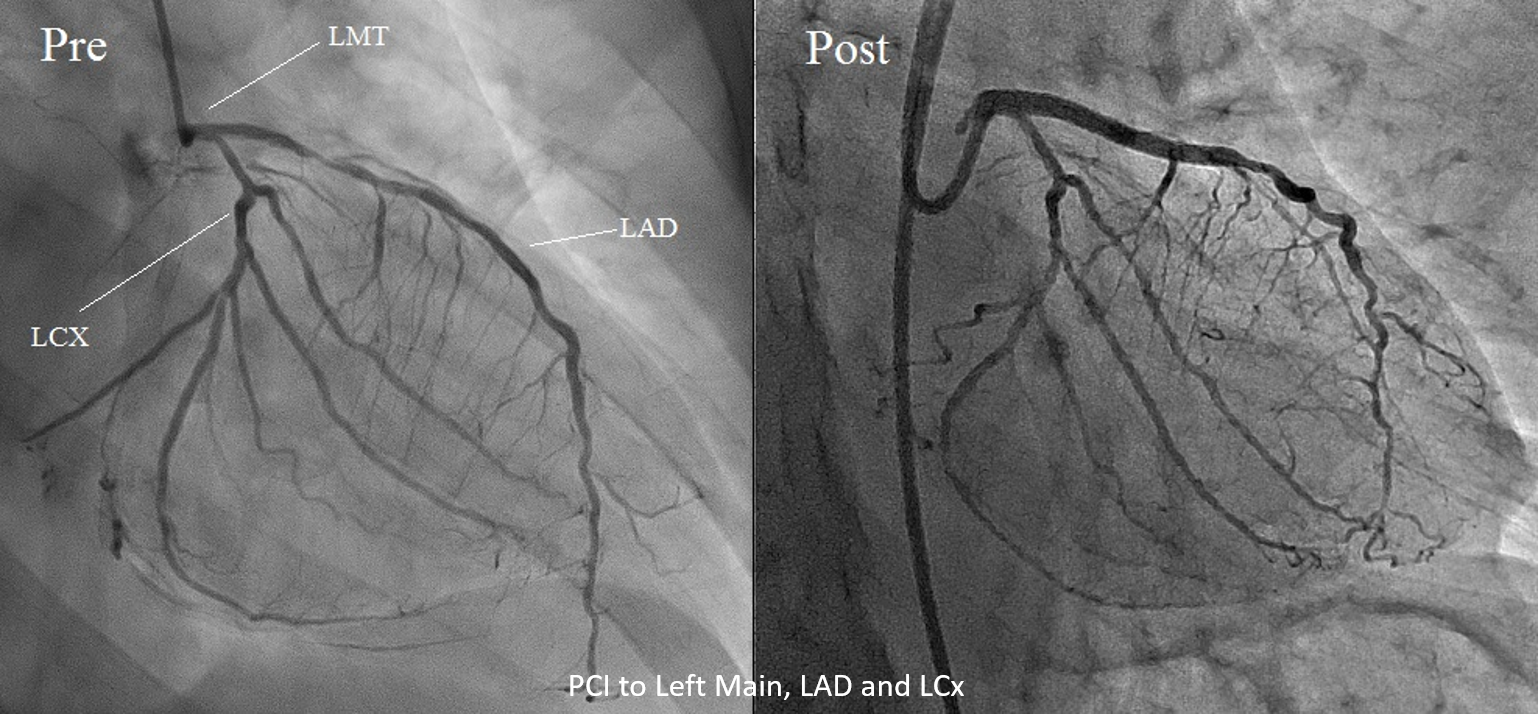 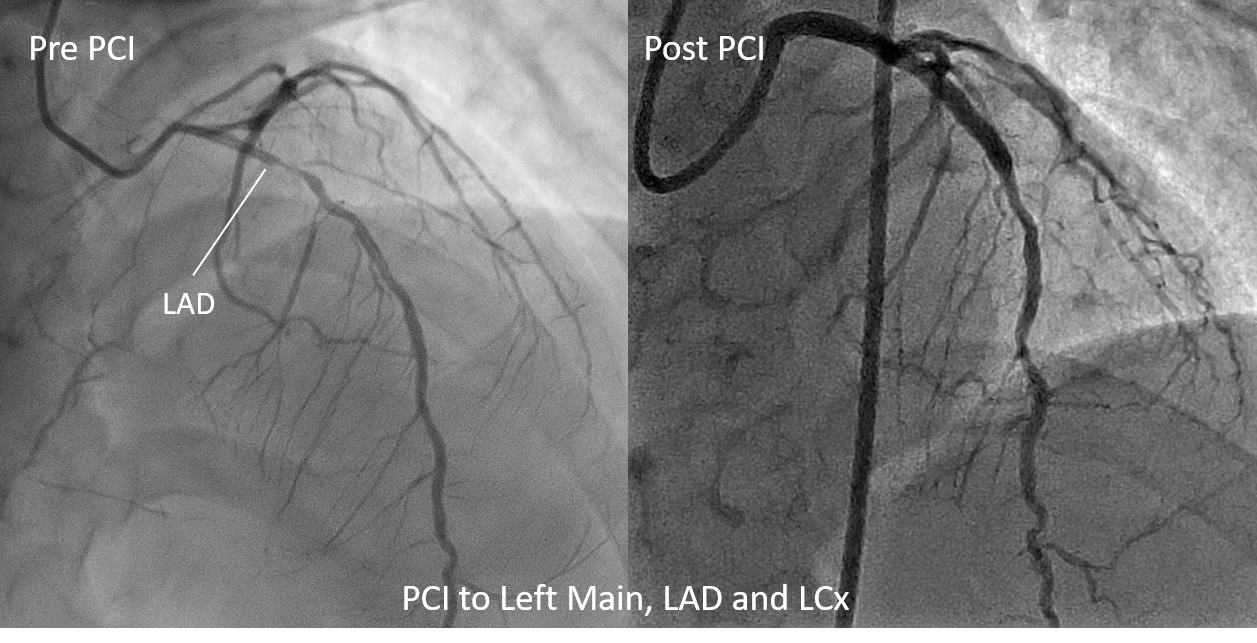 |
|
|
[Interventional Management]
- Procedural step:
J-CTO score 3. PCI strategy: antegrade wire escalation (AWE), if fail, for retrograde wire escalation (RWE).
Repeated IVUS showed good apposition of the distal RCA stent and under-expansion of previous proximal RCA stent. Proximal RCA stent was post-dilated with Emerge NC 4.0 mm x 15 mm balloon. Post PCI IVUS showed no distal stent edge dissection with good apposition of the stent. 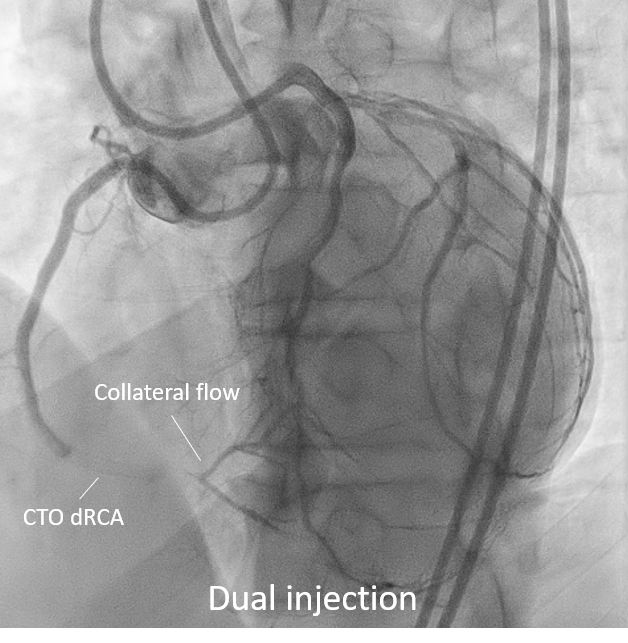 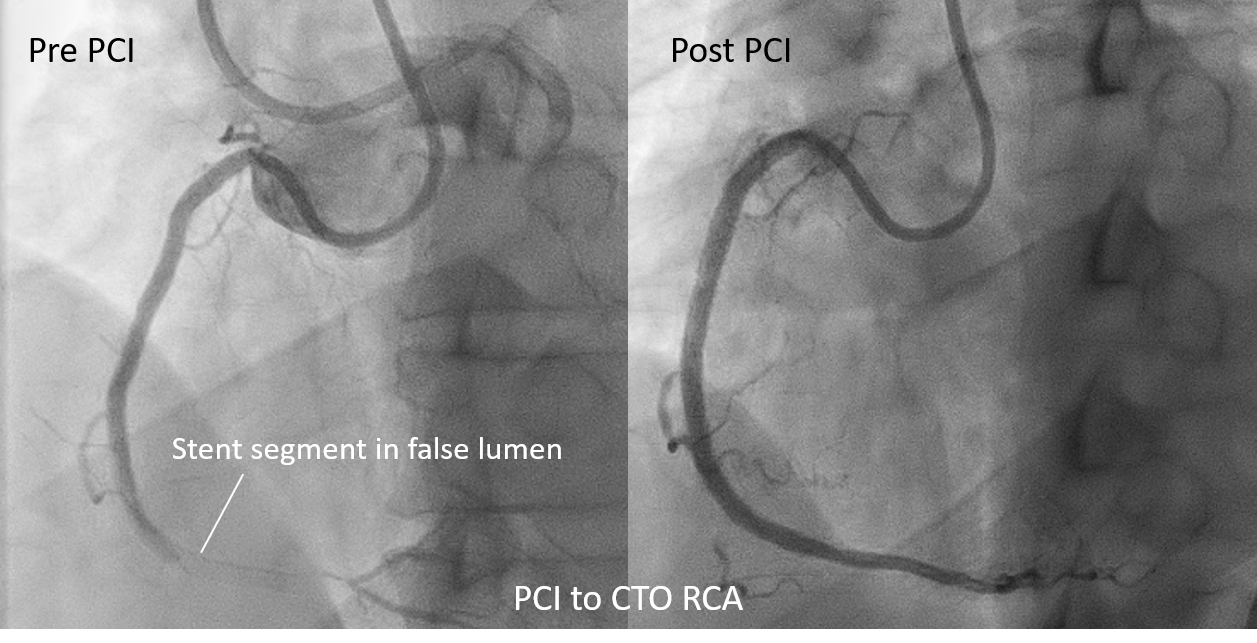 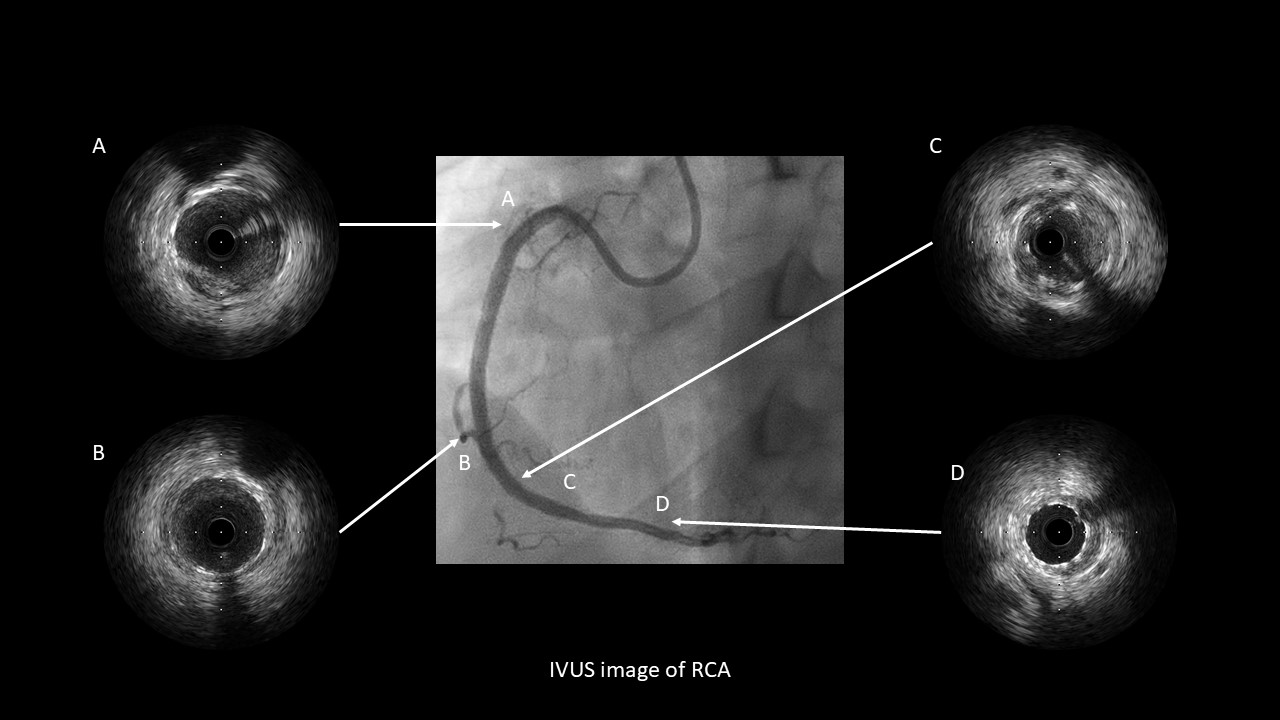 - Case Summary:
This case illustrated the danger of implanting a stent into false lumen. When the distal wire position is ambiguous in a CTO, the operator should refrain from implanting a stent without confirming that the wire is truly intraluminal either by IVUS , contralateral injection etc. However, false lumen stenting is salvageable by careful planning and applying the correct strategy in our case.
|
|