Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191021_005
| STRUCTURAL HEART DISEASE - Valvular Intervention: Mitral or Tricuspid | |
| MitraClip® Therapy for Dynamic Mitral Regurgitation with Repetitive Heart Failure Exacerbation | |
| Akiko Masumoto1, Shunsuke Kubo1, Masanobu Ohya1, Keigo Miyajima1, Koya Okabe1, Katsuya Miura1, Takeshi Maruo1, Kazushige Kadota1 | |
| Kurashiki Central Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
SO
-Relevant clinical history and physical exam:
An 89-year-old woman with a history of percutaneous coronary interventions for three-vessel coronary artery disease was admitted to hospital for heart failure (HF). She was given 5 mg per day of prednisolone for rheumatoid arthritis. On admission, her blood pressure was 130 over 70 mmHg. Systolic murmur was observed at apex, and slight pitting edema was noted on both legs.
-Relevant test results prior to catheterization:
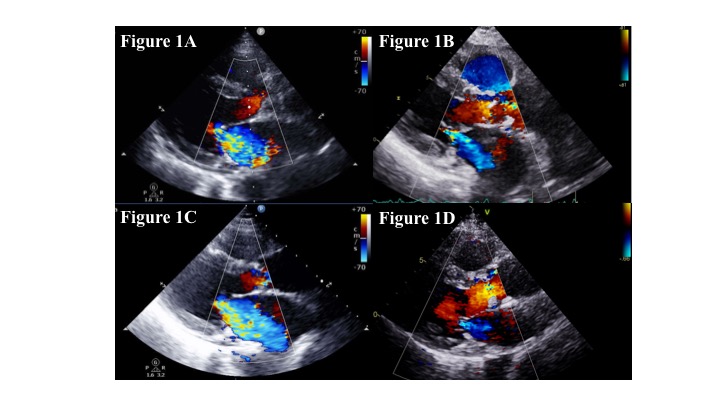
Electrocardiogram showed sinus rhythm with complete right bundle branch block, and bilateral congestion was seen on chest X-ray. Transthoracic echocardiography revealed severe mitral regurgitation (MR) with leaflets tethering (Figure 1A). The left ventricular ejection fraction was 71 %, and there was no regional wall motion abnormality.
 - Relevant catheterization findings:
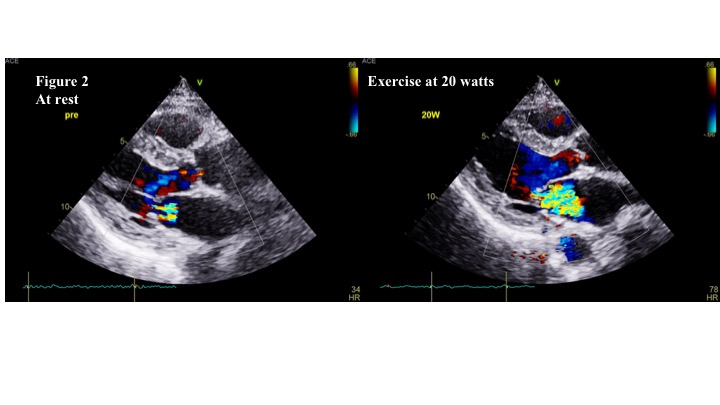
After treatment with diuretics and vasodilators, MR improved to mild (Figure 1B). However, only a week after the discharge, she was re-admitted for HF with resting dyspnea. MR had worsened to severe again, and then dynamically decreased to mild following HF treatment (Figures 1C and 1D). On stress echocardiography, MR immediately became severe with exercise at 20 watts, which we diagnosed as exercise-induced MR (Figure 2).
 |
|
|
[Interventional Management]
- Procedural step:
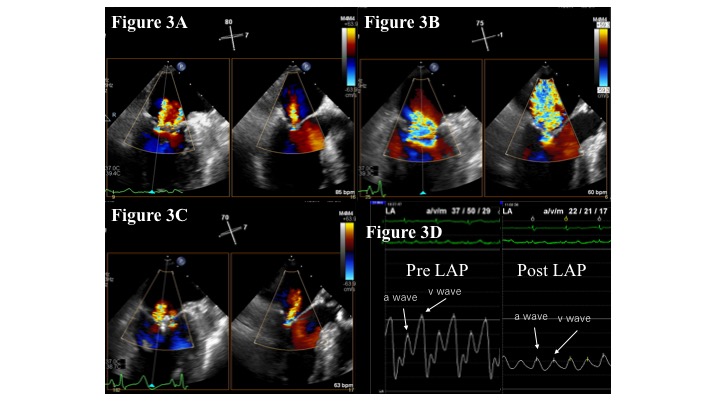
As she had repetitive episodes of HF admission and also a high operative risk, we performed MitraClip (Abbott Vascular, Santa Clara, California) implantation. Transesophageal echocardiography before the procedure showed only mild MR (Figure 3A). Because it was difficult to decide the optimal clip location and procedural endpoint of the MitraClip for this mild MR, we reproduced severe MR with fluid and norepinephrine infusion during the procedure (Figure 3B), which facilitated the successful treatment of MR with 1 clip with significant reduction in the left atrial pressure (Figures 3C and 3D). Afterwards, MR was reduced to mild, and she remained asymptomatic in NYHA Class I, without further re-hospitalization for HF.
 - Case Summary:
Dynamic MR, which is increased by HF exacerbation or exercise, is associated with increased mortality and HF re-admissions. However, it is unknown whether patients with dynamic MR would benefit from mitral valve treatment because of the less severity at rest or after HF treatment. Our case suggests that the MitraClip can be effective in improving the clinical symptoms and preventing further HF admission in patients with repetitive HF hospitalization accompanied by dynamically increased severe MR.
|
|