Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191021_002
| CORONARY - Chronic Total Occlusion | |
| Difficult RCA Chronic Total Occlusion: Choose the Right Way to Roma. | |
| Chia-Chang Lin1, Jun-Ting Liou2 | |
| Tfagh, Taiwan1, Tri-Service General Hospital, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
a 71-year-old male
-Relevant clinical history and physical exam:
A 71-year-old male patient was admitted for frequent effort chest tightness and exaggerated exertional dyspnea for 2 months. That chest discomfort could be partially relieved by sublingual NTG. He underwent PCI with bare-metal stenting at both left circumflex artery and right coronary artery 11 years ago. His coronary risk factors were hypertension, type 2 diabetes mellitus and dyslipidemia. No significant abnormality of physical exam.
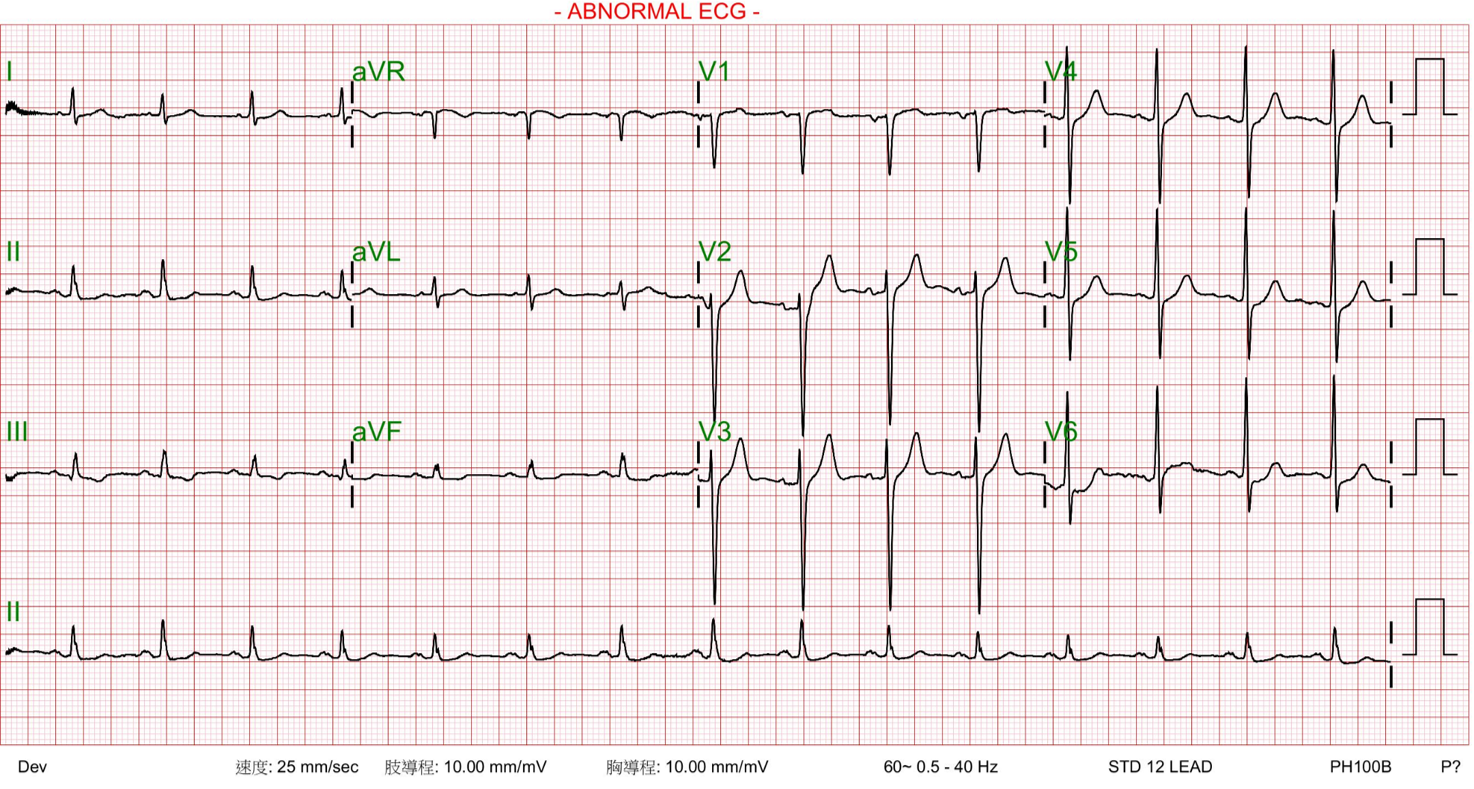
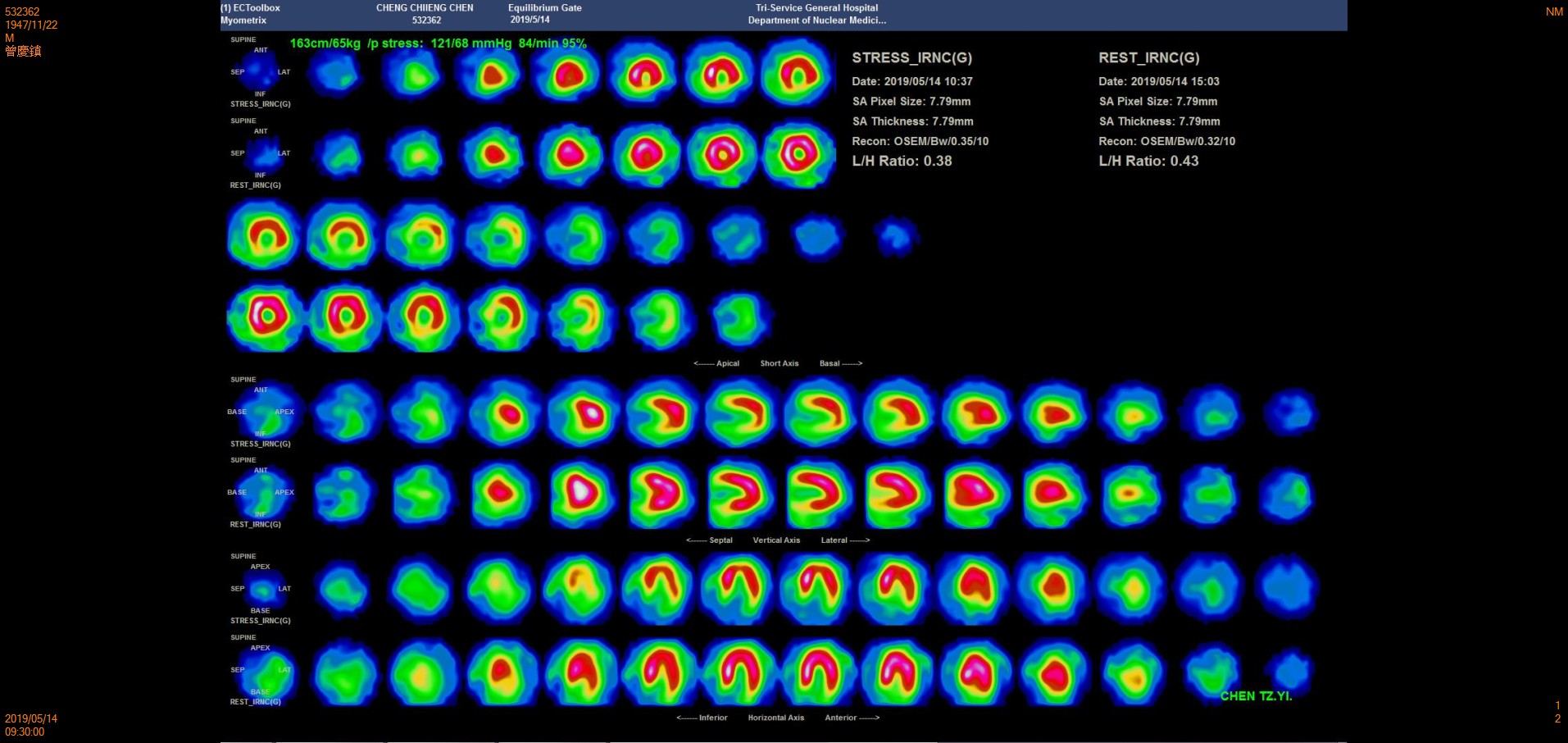
-Relevant test results prior to catheterization:
His electrocardiogram(ECG) demonstrated left ventricular hypertrophy and T wave inversion of lead III& aVf. Echocardiography showed normal ejection fraction without regional wallmotion abnormalities. Tl-201 myocardial perfusion scan revealed severeischemia at inferior wall of the left ventricle ( suggest hypo-perfusion degree65~70 % of RCA territories).
   - Relevant catheterization findings:
Left coronaryangiogram showed significant stenosis from proximal to middle part of leftanterior descending (LAD). De novo tandem lesions at proximal and distal leftcircumflex artery (LCX). Both LAD and LCX gave collateral flow to rightcoronary artery territory (RCA).
|
|
|
[Interventional Management]
- Procedural step:
7 Fr sheathes were inserted thorough right radial and right femoral artery. Left coronary artery was engaged with a 7 Fr EBU 3.5 guide catheter. RCA was engaged with a 7 Fr SAL-1 guide catheter. We took wire escalation strategy and tried to antegradely cross the distal RCA CTO body with the help of Caravel 135 cm microcatheter but all wires entered to sub-intimal space. Thus we shifted to retrograde approach. We selected one collateral channel from LCX to PDA owing to more obvious on angiography and the least tortuosity. After several attempts, we successfully enter distal PDA segment via SION wire plus Caravel 150cm microcatheter. Then we shifted the wire to Gaia II but could not findtrue tract back to d-RCA. After several failed attempts, we decided to implement Reversed CART technique and successfully shifted wire to RG-3. After IVUS evaluation, we pre-dilated the RCA CTO lesions with a 3.0x20 mm Tazuna balloonand a 3.5x20 mm Accuforce NC balloon at proximal to middle RCA lesion. A 2.5x48 mm Xience-Xpidition DES was properly deployed at distal RCA, crossing to the proximal portion of PDA and a 3.5x48 mm Xience-Xpidition DES was deployed at proximal to middle portion of RCA. Then post-dilatation was implemented with 3.0x20 mm Tazuna balloon at distal RCA and 3.5x20 mm Accuforce NC balloon at proximal RCA. The uncovered previous stent segment was then treated by a 3.5x20 mm Dior DCB. Final angiography and IVUS showed that the procedure was successful.
- Case Summary:
1. The rate of BMS-ISR is high, especially in multiple coronary risk factors group
|
|