Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191019_003
| CORONARY - Chronic Total Occlusion | |
| Successful Bail-Out from Perforation in Long RCA-CTO | |
| Takuma Tsuda1 | |
| Nagoya Ekisaikai Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
N.T.
-Relevant clinical history and physical exam:
Age:55y
 -Relevant test results prior to catheterization:
ECGshowed abnormal Q wave in Ⅱ,Ⅲ,aVF and poor R wave in V3-5
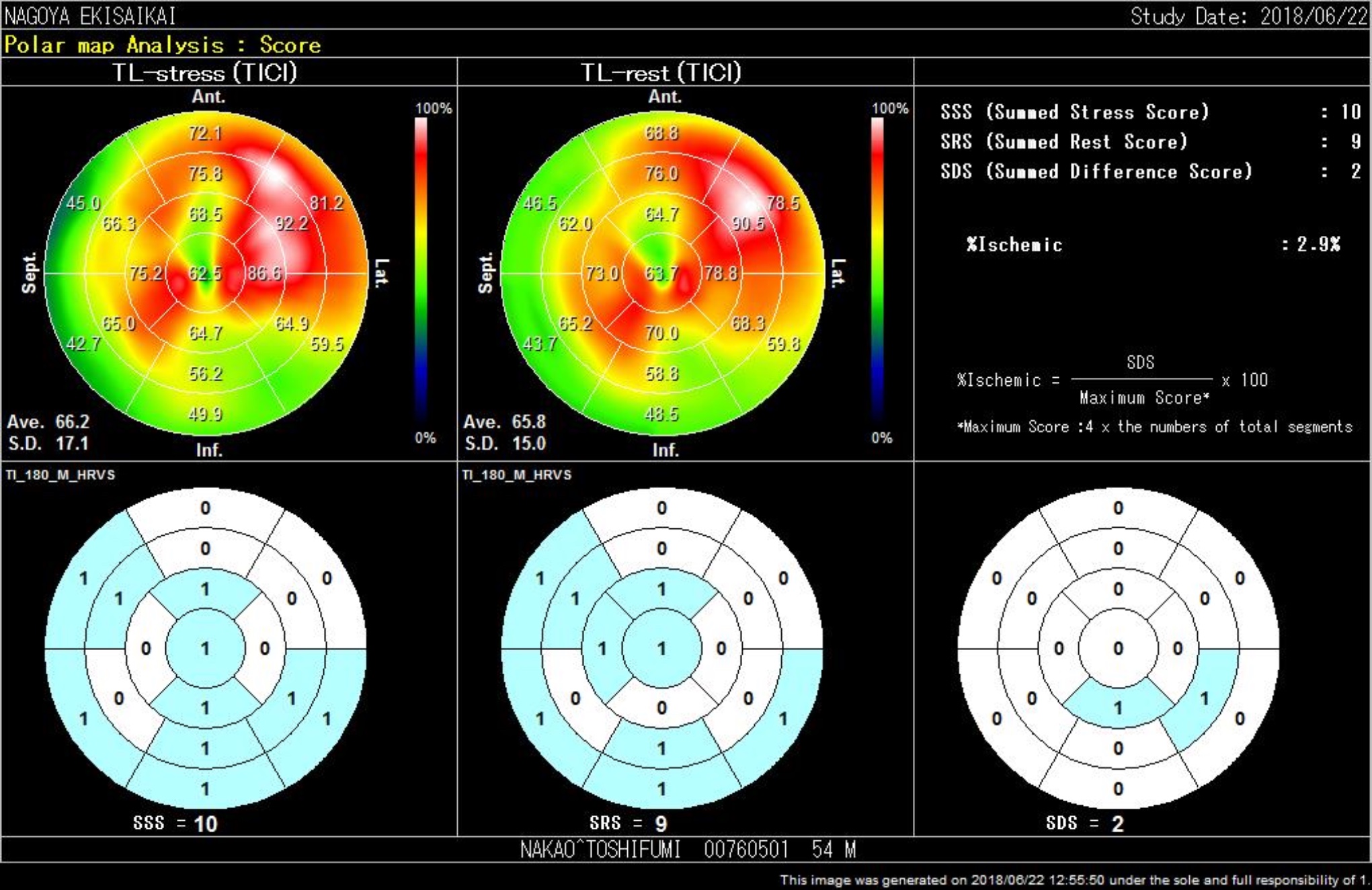
CT showed long RCA-CTO with a few calcification MPI showed positive viability of inferior wall 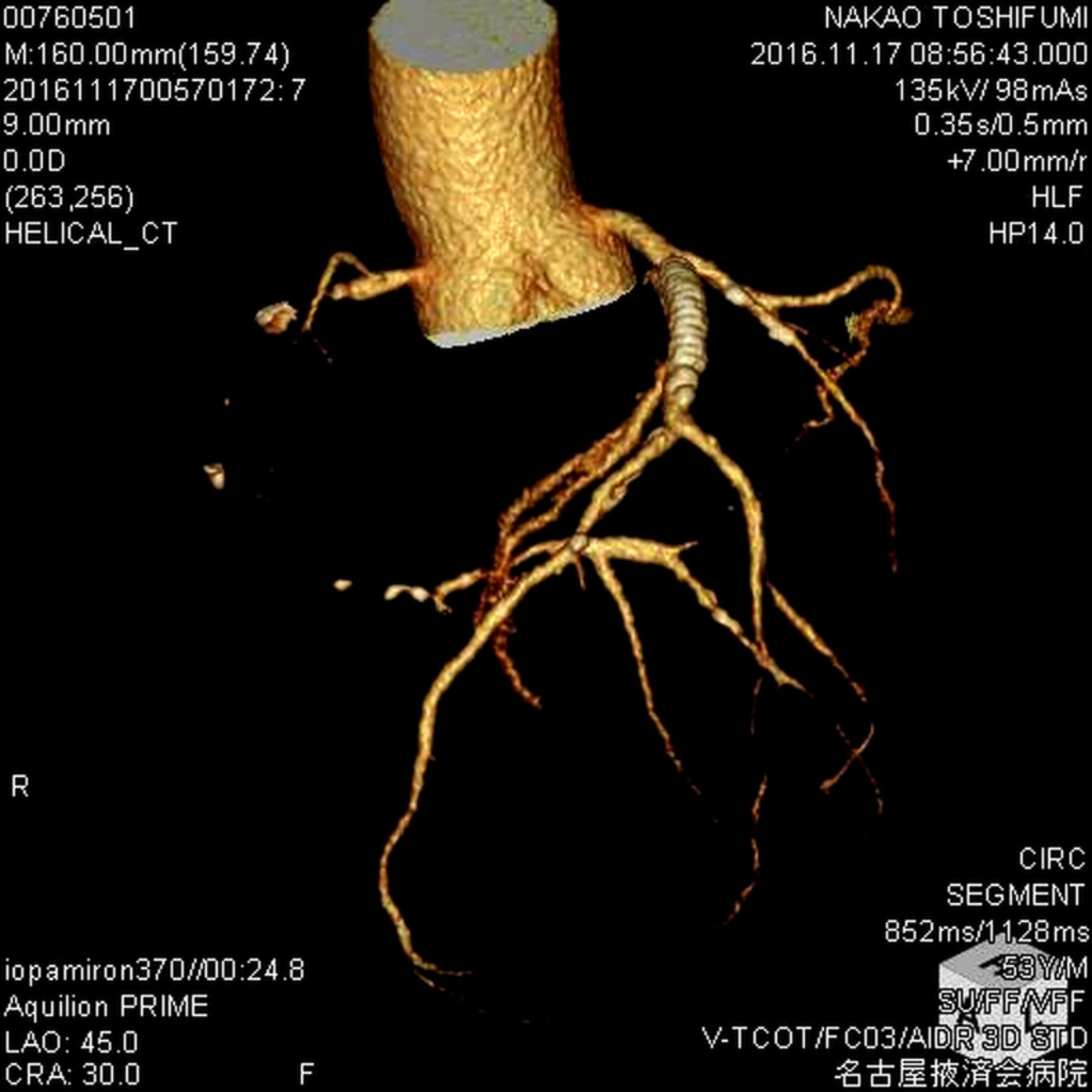 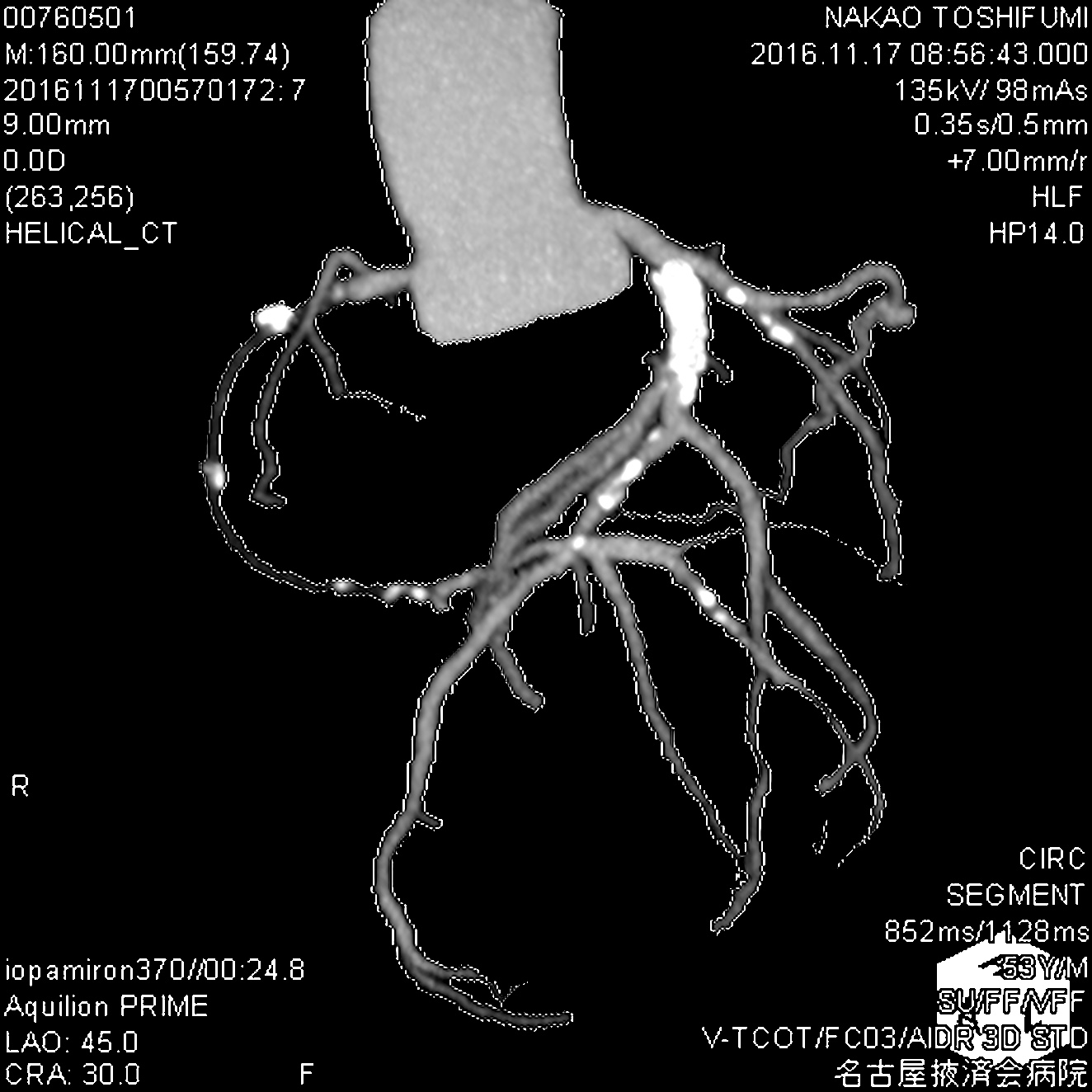  - Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
1. 1st retro 2. retrograde wiring
5. antegrade wiring 10. POBA/stenting(#2:perforation site) 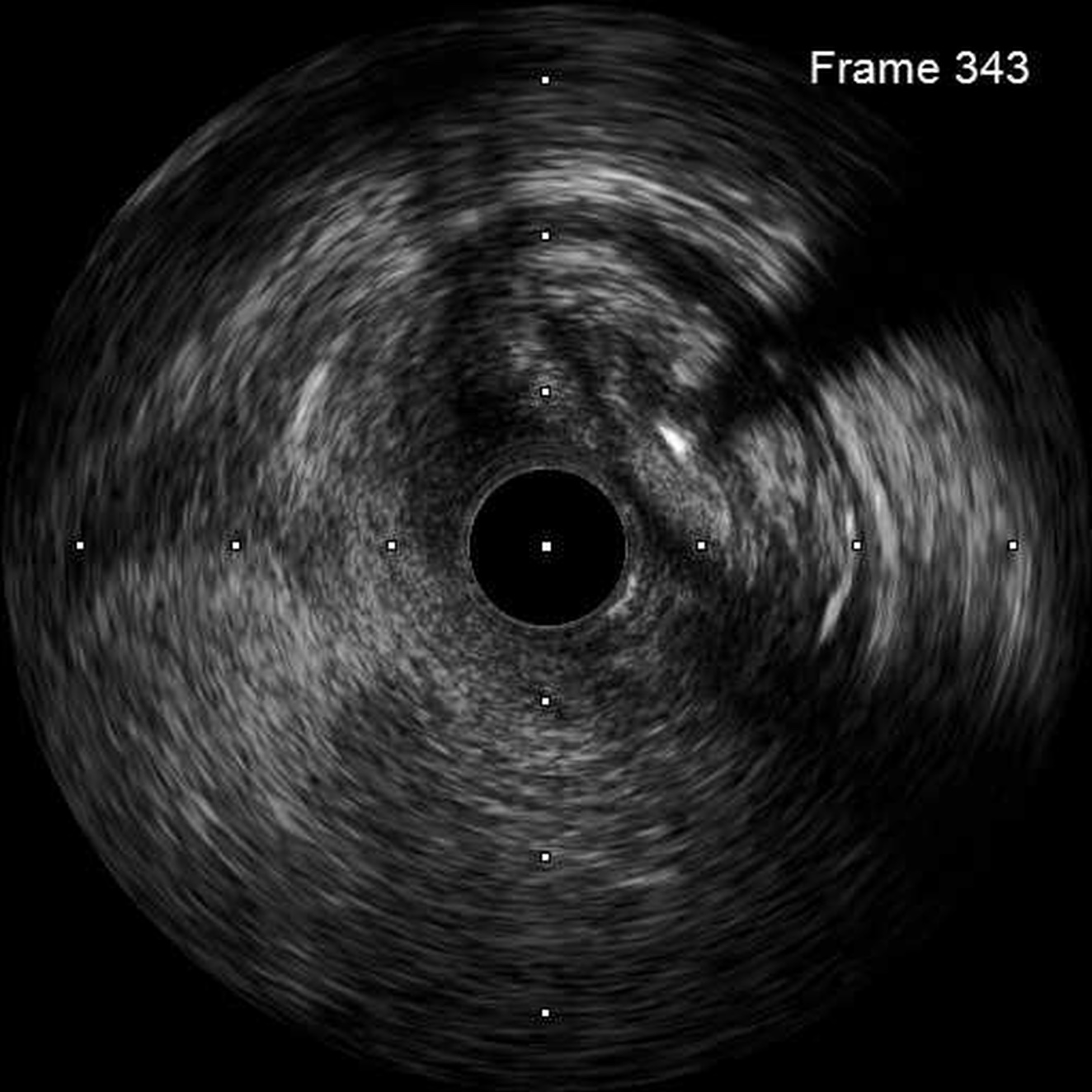 - Case Summary:
CTO sometimes has risk of perforation. I performed atypical but representative and educational methods for bail-out of perforation under imaging modality. However we also know much more options for overcoming this kind of situations. Here I will show the importance of the way to use imaging modality even in CTO after externalization.
|
|