Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191018_002
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Cardiogenic Shock Complicating Ostial Left Anterior Descending Artery STEMI with Chronic Total Occlusion Left Circumflex Artery | |
| Korakoth Towashiraporn | |
| , | |
|
[Clinical Information]
- Patient initials or identifier number:
PS
-Relevant clinical history and physical exam:
A 52-year-old man with type II diabetes and hypertension, visited our emergency department because of angina for 2 hours. On examination the blood pressure was 89/54 mmHg.,the heart rate was 114 beats perminute, the respiratory rate was 24 per minute and the oxygen saturation was 99%.
-Relevant test results prior to catheterization:
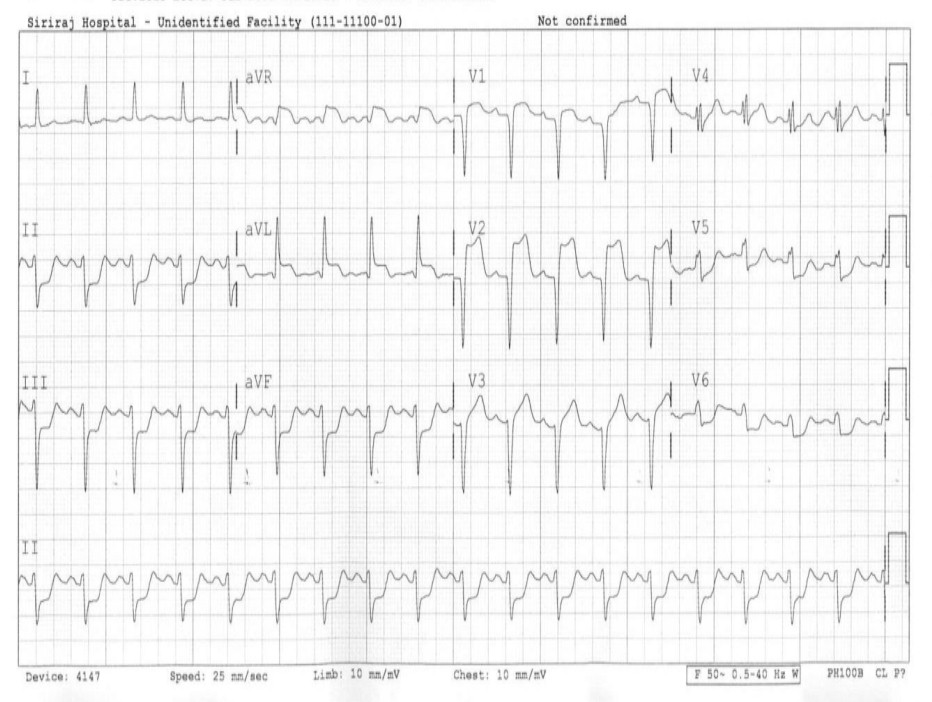
A 12-leads ECG demonstrated sinus tachycardia at a rate of 110 beats per minute. There was ST segment elevation in leads V1-V3, aVL and aVR with reciprocal changed in leads II,III,aVF, V5 and V6.
 - Relevant catheterization findings:
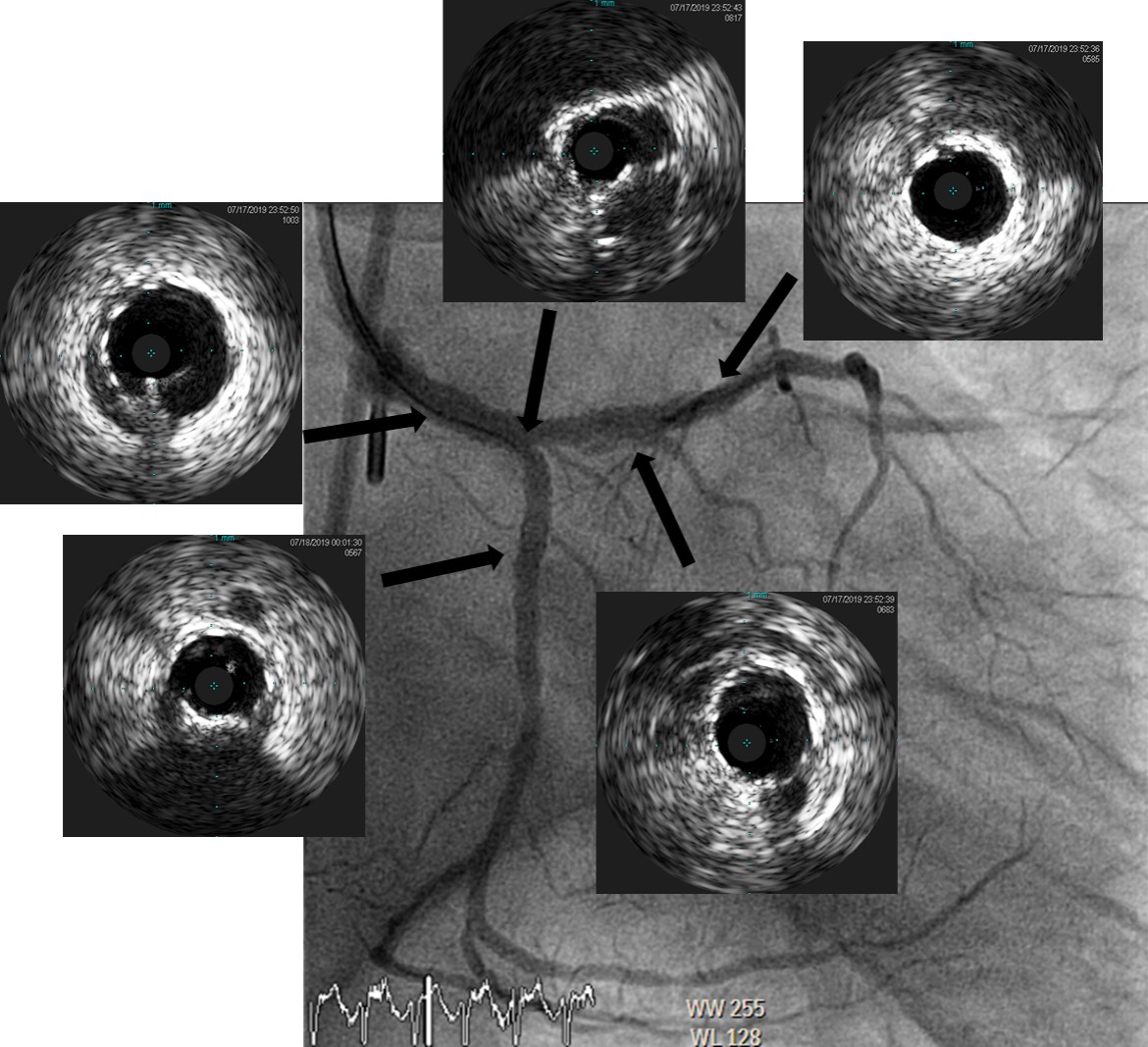
6Fr. vascular sheath was inserted into right femoral artery.Coronary angiogram (CAG) revealed left main coronary artery (LMCA) had 70%stenosis at distal part. There was 90% stenosis at ostial left anterior descending (LAD) artery with total occlusion at proximal LAD. There was 95%total occlusion at proximal left circumflex (LCX) artery with total occlusion at mid LCX. There was 80% diffuse stenosis at co-dominant proximal right coronary artery(RCA).
|
|
|
[Interventional Management]
- Procedural step:
-7Fr Extra-backup guide catheter (Medtronic Inc., USA) wasengaged to ostial LMCA.
 - Case Summary:
- Cardiogenic shock complicating ST-segment elevation myocardial infarction (STEMI) has a high mortality rate. This situation required emergent revascularization of culprit vessel, vasopressor drugs, mechanical circulatory support, and intensive care post catheterization. - We demonstrated STEMI patient with cardiogenic shock treated with primary PCI for LMCA bifurcation including PCI of chronic total occlusion (CTO) co-dominant LCX.
|
|