Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191017_003
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Non-Invasive | |
| Multimodality Imaging in an Unusual Case of Angina: Calcified Fusiform Aneurysmal Dilatation of Coronaries | |
| Patrick WJ Tiau1 | |
| Sunway Medical Centre, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
MF
-Relevant clinical history and physical exam:
27-year-old gentleman presented with central chest pain upon exertion. Past medical history include history of myocardial infarction four years ago.There were absence of cardiovascular risk factors such as family history premature CAD, cigaretes smoking or other co-morbidity.
Clinically he was stable without signs of heart failure.Cardiovascular and other systemic examinations were unremarkable. ECG showed sinus rhythm with no significant.Serial troponin I were all negative. -Relevant test results prior to catheterization:
Transthoracic echocardiogram showed good LV systolic function.There was absence of regional motion wall abnormality.Parasternal short axis at aortic valve showed an echolucent area adjacent to the left coronary origin, which more apparent on focus viewHowever there was absence of signal in colour doppler flow.
Patient was planned for Calcium score and CT coronary angiogram 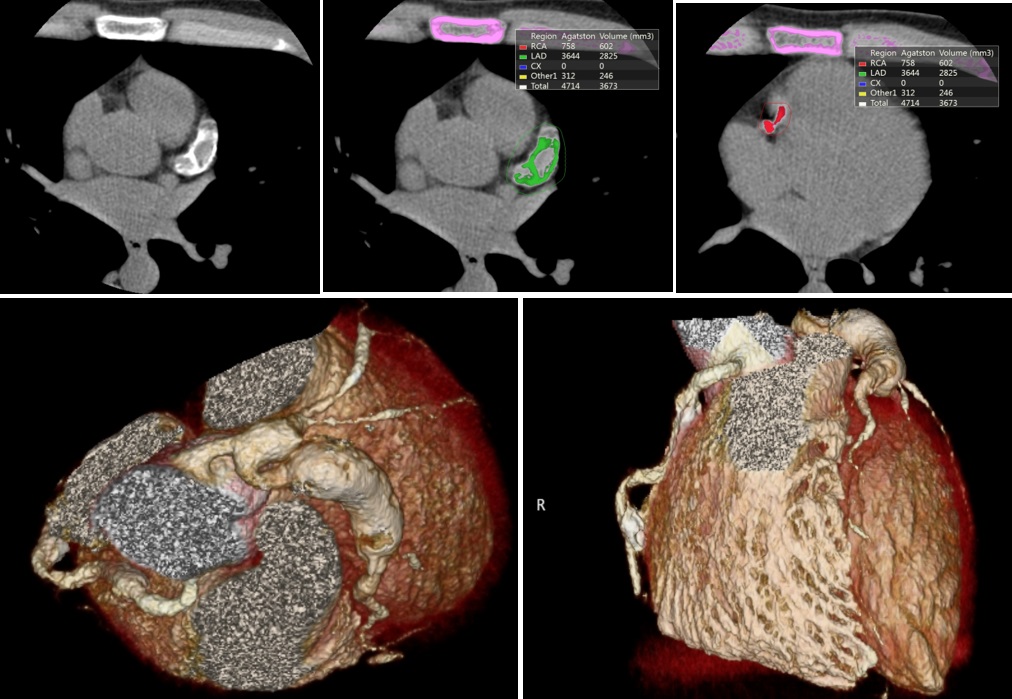 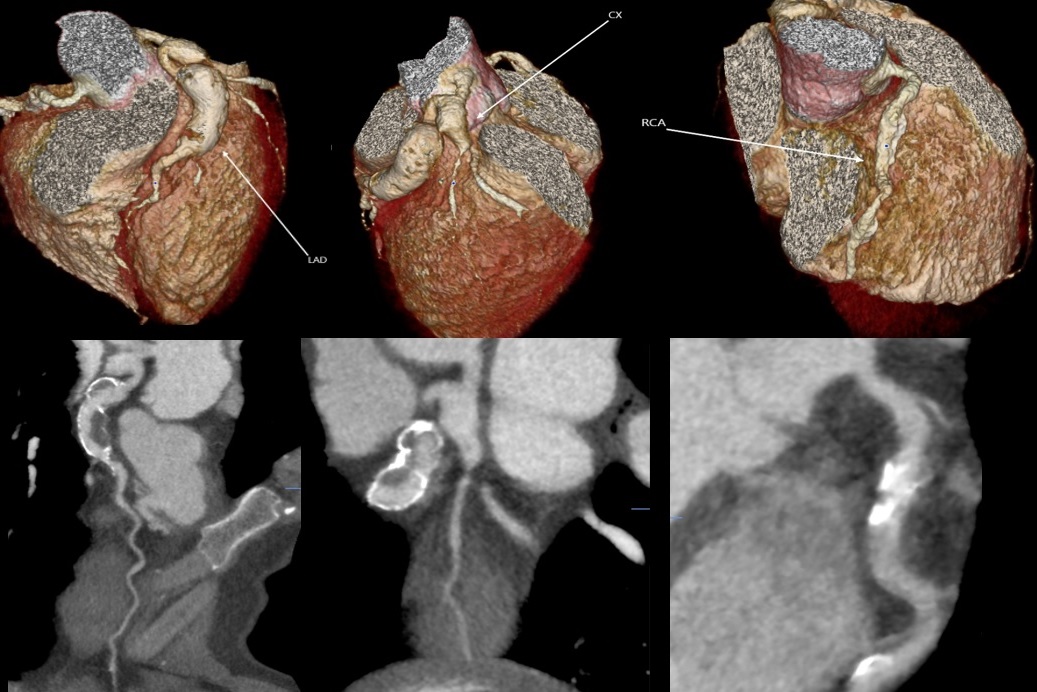 - Relevant catheterization findings:
COROS : Mid to distal left main severe aneurysmal dilatation up to 12mm by QCA, Calcified proximal aneurysmal dilatation of LAD with contrast filling defect , followed by torturous vessel distally with TIMI II flow Extension of aneursymal from LM to LCx followed by tortuous vessel distallyDiffuse ectacsia of RCA with slow flow
 |
|
|
[Interventional Management]
- Procedural step:
Area of perfusion defect was evidenced by SPECT perfusion scan.
A conjoint team discussion with the patient and cardiothoracic team was done to determine the optimal management, considering the aneurysmal's size and slow flow which was associated with high risk thrombogenicity and subsequent cardiac event. Surgical revascularization is preferred here considering the size and anatomical location of the aneurysm involved the distal left main, which was not favorable for percutaneous coronary intervention (covered stent, double layer BMS) Hence, patient is planned for CABG with aneurysmal ligation followed by LIMA to LAD and SVG to OM/LCx. 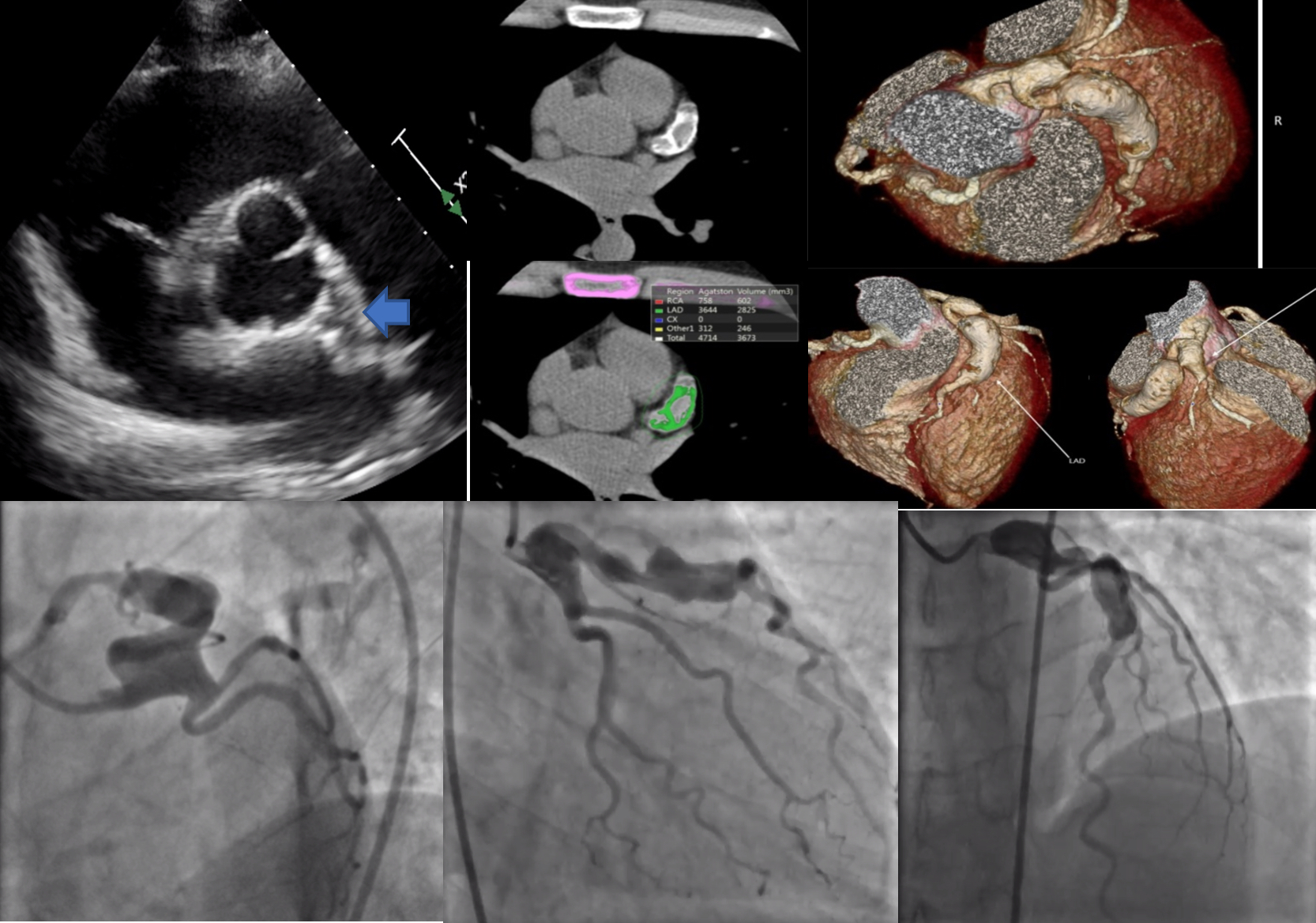 - Case Summary:
The diagnosis and the accurate anatomical mapping of the coronary aneurysm made by both non-invasive and invasive multimodality imaging here is invaluable, which subsequently help to determine the optimal mode of revascularization and has resulted in a favourable clinical outcome.
|
|