Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191017_002
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| The Curious Case of Cracked Coronaries | |
| Thurston Erng1, Kamaraj Selvaraj2 | |
| Serdang Heart Centre, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
JG
-Relevant clinical history and physical exam:
A 45 year old male with underlying HIV infection on HAART presented with chest pain for 2 days associated with dyspnoea. Diagnosis of NSTEMI with transient complete heart block was made based on clinical investigations. Despite initial medical therapy, intermittent chest pain persisted and he was transferred emergently to our centre for coronary angiography.
-Relevant test results prior to catheterization:
5 months prior to current presentation, he was admitted to the same non-PCI centre with posterior myocardial infarction complicated by cardiogenic shock (Killip IV) and resuscitated ventricular fibrillation (VF). At the time, he received intravenous streptokinase thrombolysis and standard STEMI medical therapy but declined invasive coronary angiography. He recovered well and subsequently defaulted on his cardiology follow-up until the current encounter.
- Relevant catheterization findings:
Coronary angiography demonstrated eccentric, ambiguous, multi-linear lesions in both RCA and LAD with TIMI flow grade II. In particular, proximal LAD had a 'cracked' vessel appearance. LCX artery was non-dominant and angiographically normal.
Differentials at this stage included coronary artery dissection, acute thrombus, ulcerated atheromatous plaque or complex calcified lesion. 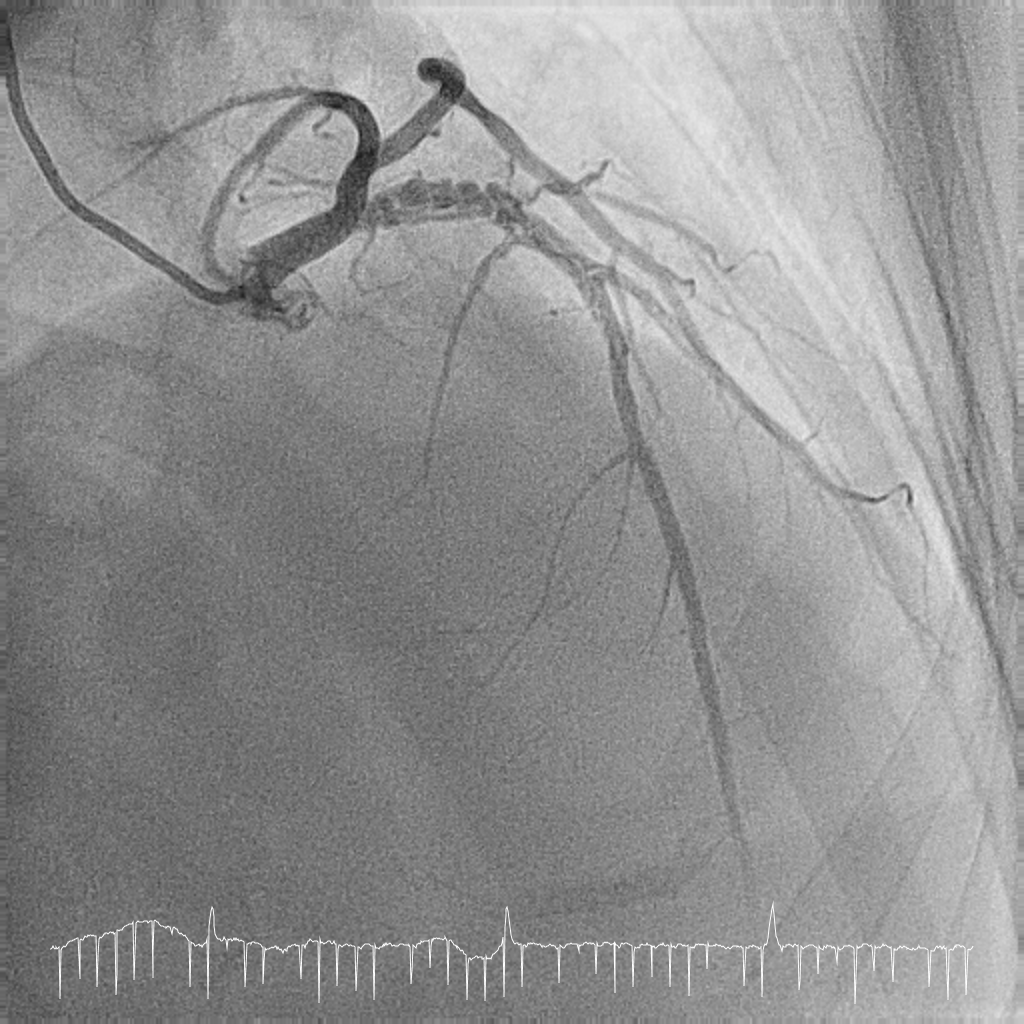 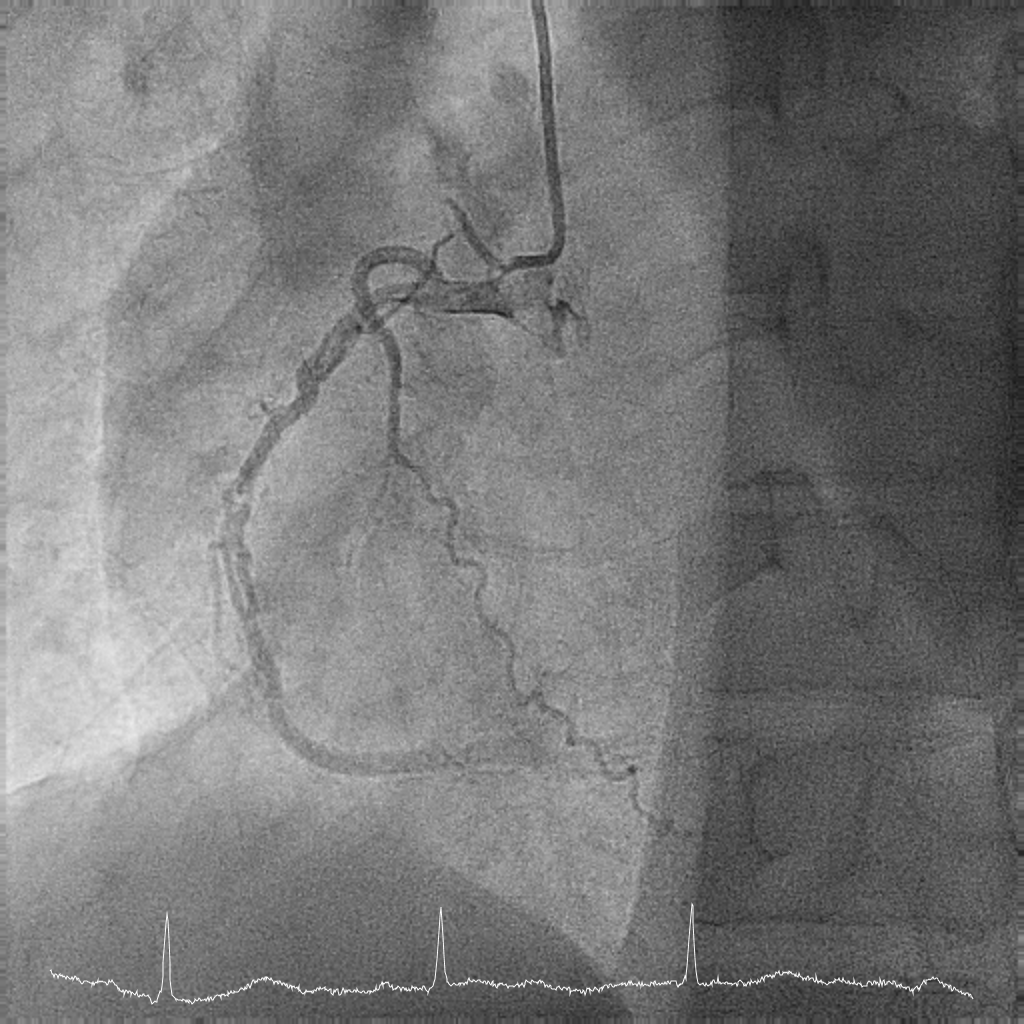 |
|
|
[Interventional Management]
- Procedural step:
We elected to perform urgent PCI to RCA due to NSTEMI with transient complete heart block and recurrent ACS. RCA was engaged with JR 3.5. Coronary wiring was carefully attempted with Fielder XT-R in Finecross microcatheter. Sequential predilation was done with Sapphire II NC 2.5 X 15 mm. 3 Zotarolimus DES were implanted – Resolute Onyx 3.5 x 30 mm, 4.0x 38 mm and 4.0 x 15 mm. Postdilation was done with Accuforce NC 3.5 X 15 mm and 4.0 x 15 mm. Good angiographic results were obtained with TIMI III flow.
We then engaged the left system with EBU 3.0. LAD was successfully wired with GAIA-1 in Finecross microcatheter and changed to Rinato wire. Optical Coherence Tomography (OCT) study of LAD was then performed demonstrating multiple channels of variable sizes, separated by thin septa of high signal intensity. The channels appear to communicate and surround a larger central lumen. At both proximal and distal ends, they coalesce into a single lumen. Residual thrombus, atheroma with possible plaque rupture and disrupted septa could also be visualized. These OCT morphologies correspond with unanticipated chronic recanalization of organized thrombus (RCT). PCI of LAD was then done with sequential predilation using Pantera LEO NC 3.0 x 15 mm. 2 Sirolimus DES were implanted - Amazonia Sir 3.0 x 28 mm and 3.5 x 28 mm. Postdilation was done with Accuforce NC 3.5 x 15 mm and 4.0 x 15 mm. Repeat OCT demonstrated excellent stent apposition with obliteration of the multiple channels. 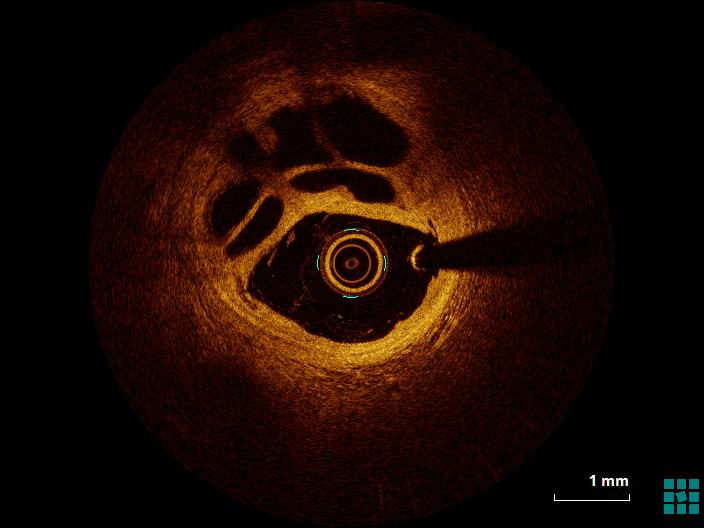 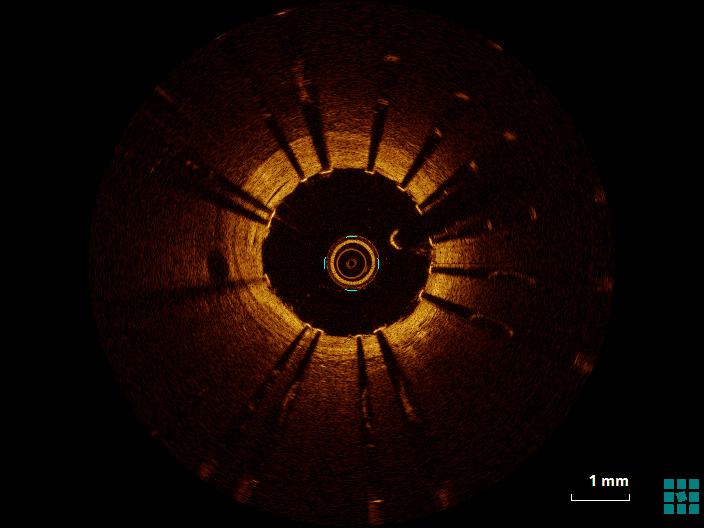 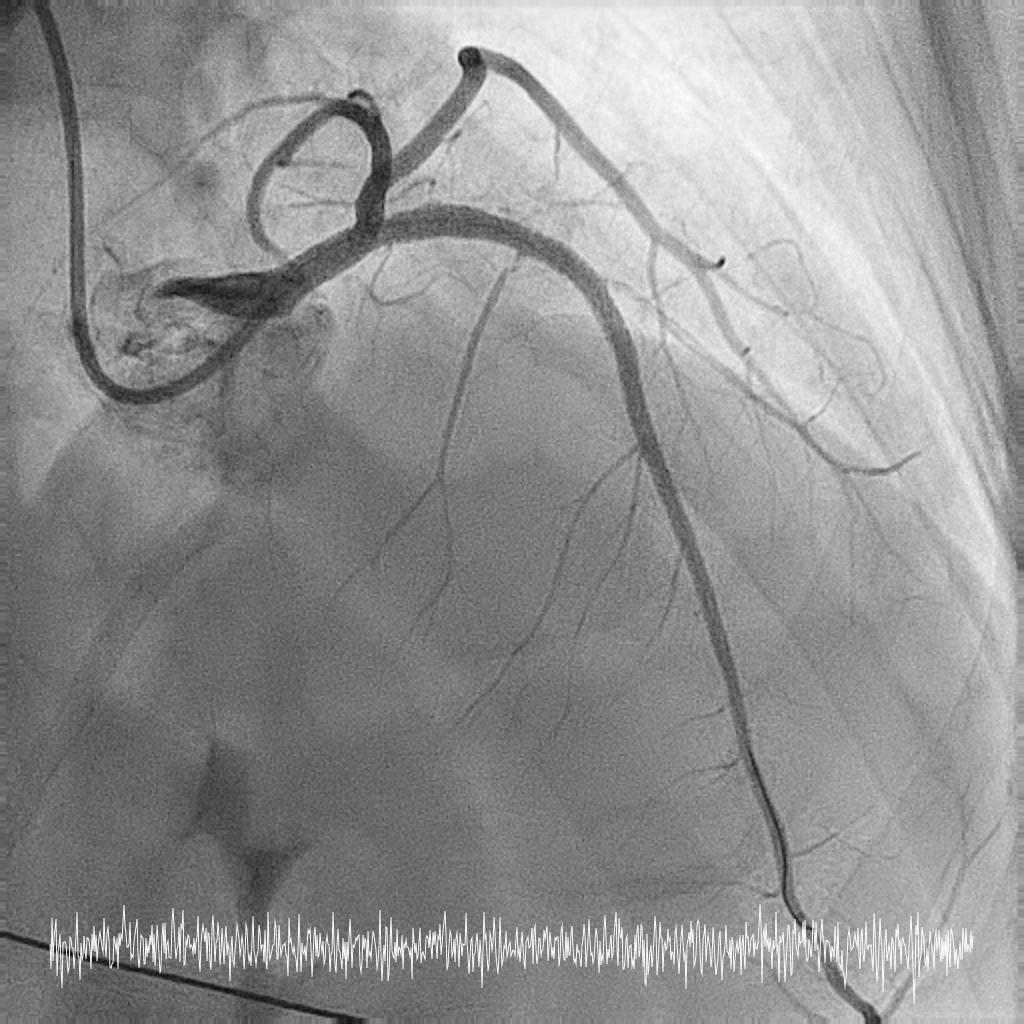 - Case Summary:
This case underscores various interesting features of a rare entity - multivessel chronic recanalization of organized thrombus (RCT) - 5 months after MI with thrombolysis in a HIV patient. Review of angiography showed features of pseudo-dissection, veiled appearance and braided characteristics which are associated with RCT. Additionally, OCT application was crucial in 5 aspects:(1) Clinching precise diagnosis of RCT(2) Visualizing areas of marked lumen compromise not appreciated on angiography(3) Suggesting possible aetiology of initial thrombus formation(4) Providing insight into lesion complexity(5) Assuring optimal PCI result of good stent apposition with obliteration of septated channels.
|
|