Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191014_007
| CORONARY - Chronic Total Occlusion | |
| Re-Approach of a Chronic Total Occlusion from Orifice of Left Anterior Descending Artery: More than Crossing It! | |
| Jia-Ling Lin1 | |
| National Cheng Kung University Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
06668536
-Relevant clinical history and physical exam:
A 43-year-old malenon-smoker with hypertension and dyslipidemia reported intermittent chesttightness for about 6 months. After evaluation, he received coronaryangiography at another hospital. It showed triple-vessel-disease, with chronictotal occlusion since orifice of left anterior descending artery (LAD).Percutaneous intervention for LAD failed so he was referred to our hospital. Weoptimized his medication but he was still symptomatic.
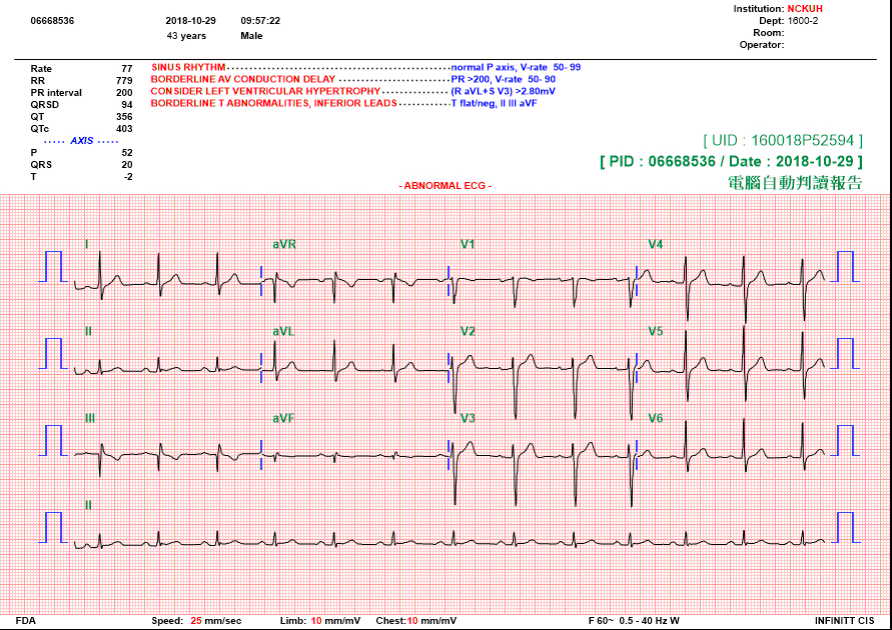
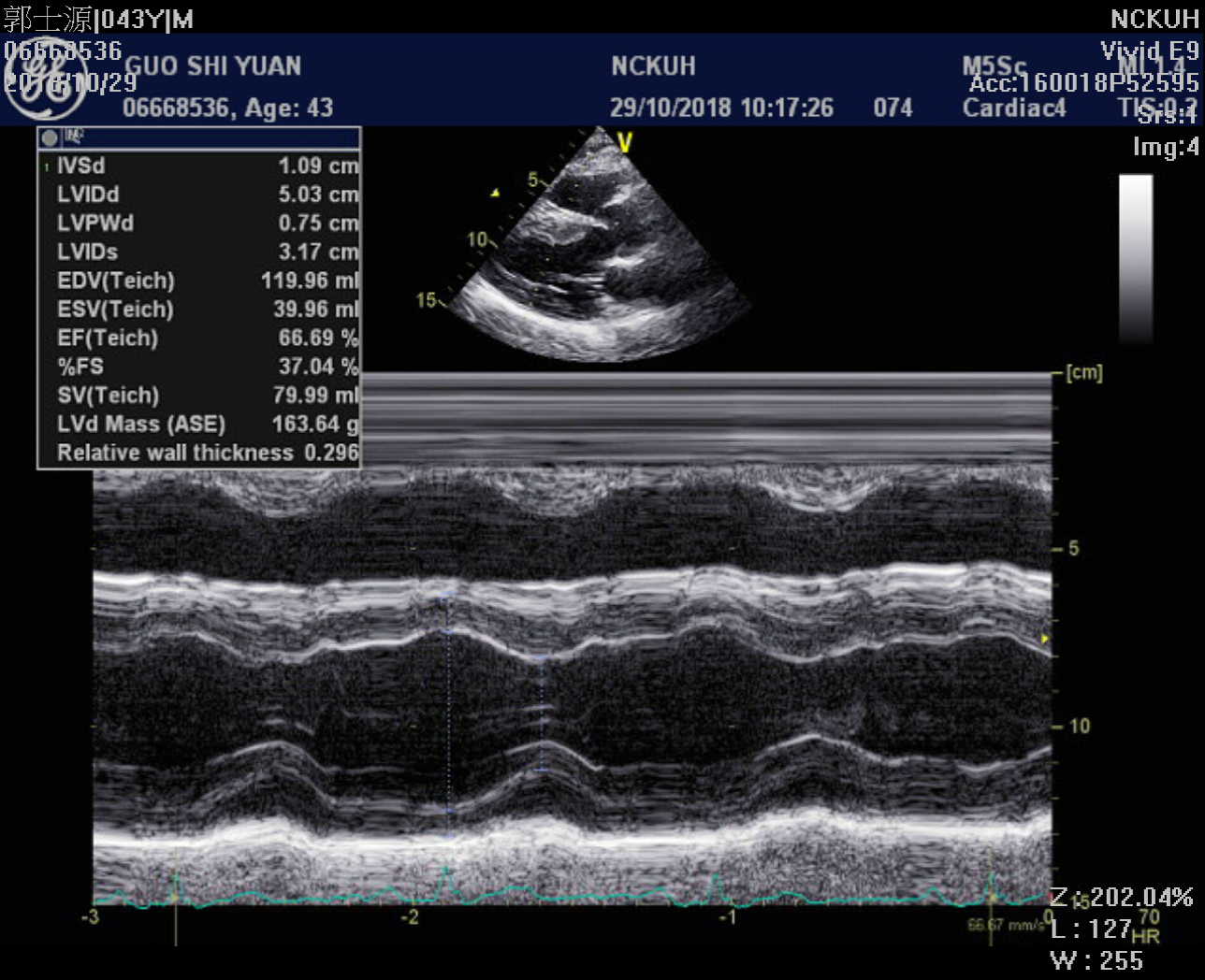
-Relevant test results prior to catheterization:
His ECG showed sinus rhythm, withnon-specific T wave change in inferior leads Echocardiography showed left ventricularhypertrophy, with adequate left ventricular systolic function.
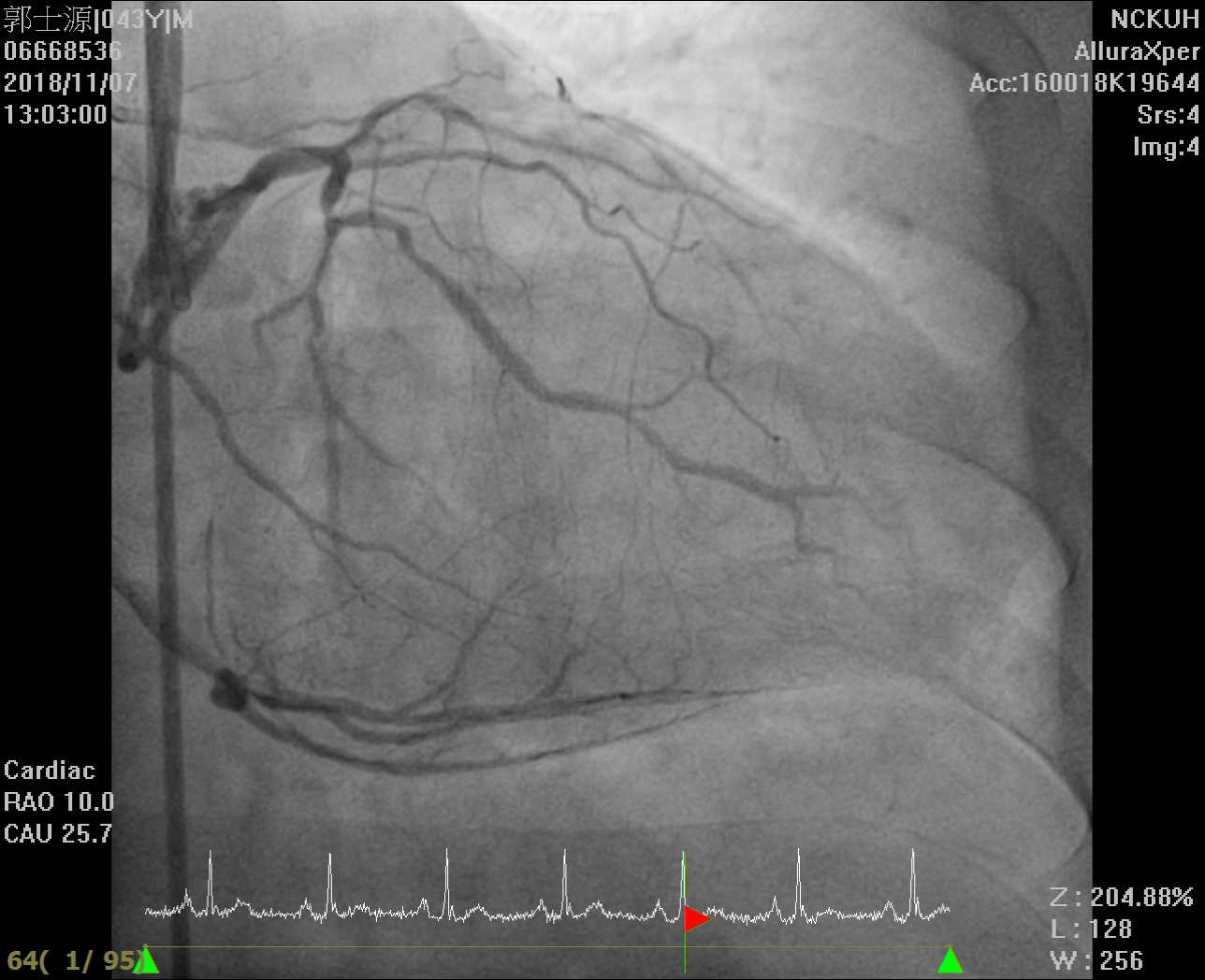
  - Relevant catheterization findings:
Coronary angiography showed triple-vessel-disease: CTO since orifice of LAD, about 70-80% stenosis at LCX and 70-80% stenosis at RCA. The CTO part was long, from proximal to middle LAD. There were collateral channels from RCA to LAD.
   |
|
|
[Interventional Management]
- Procedural step:
1. EBU4 for antegrade; SAL1(SH) for retrograde.
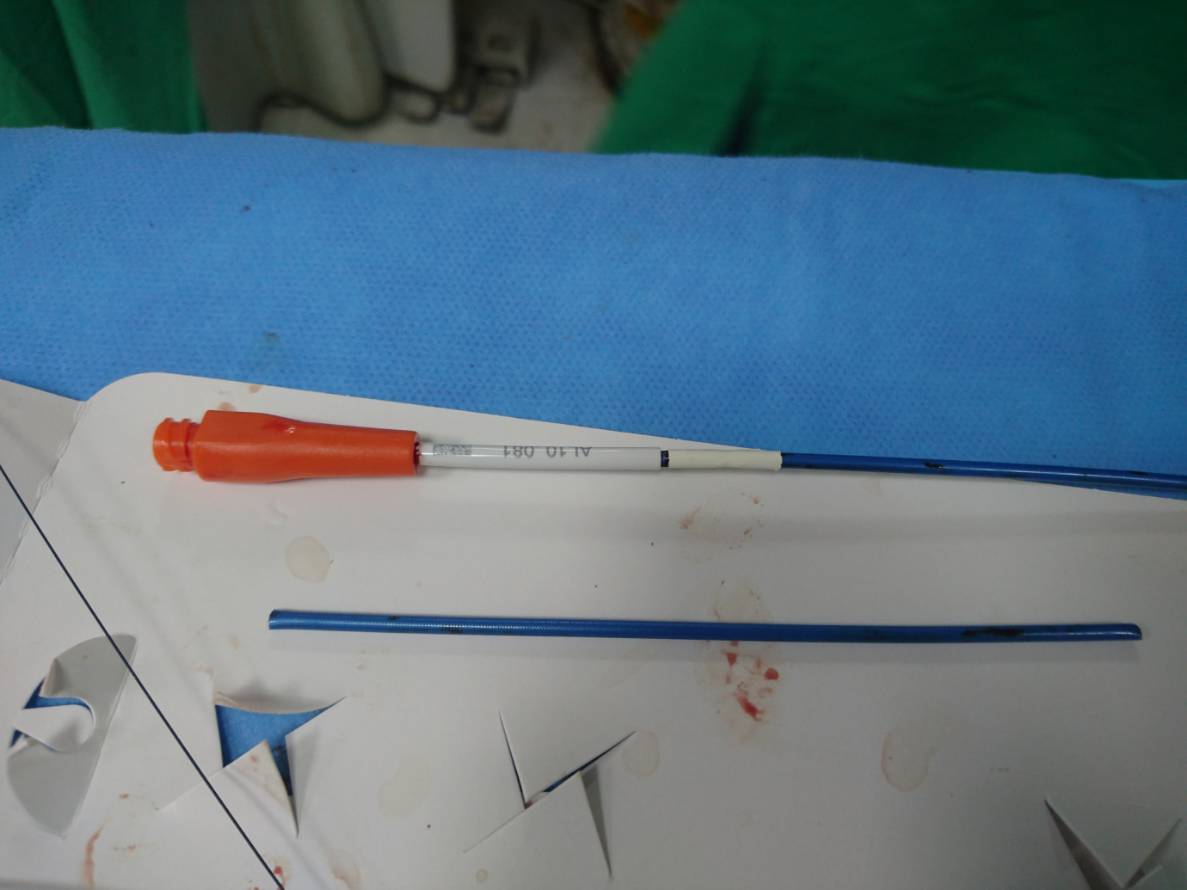 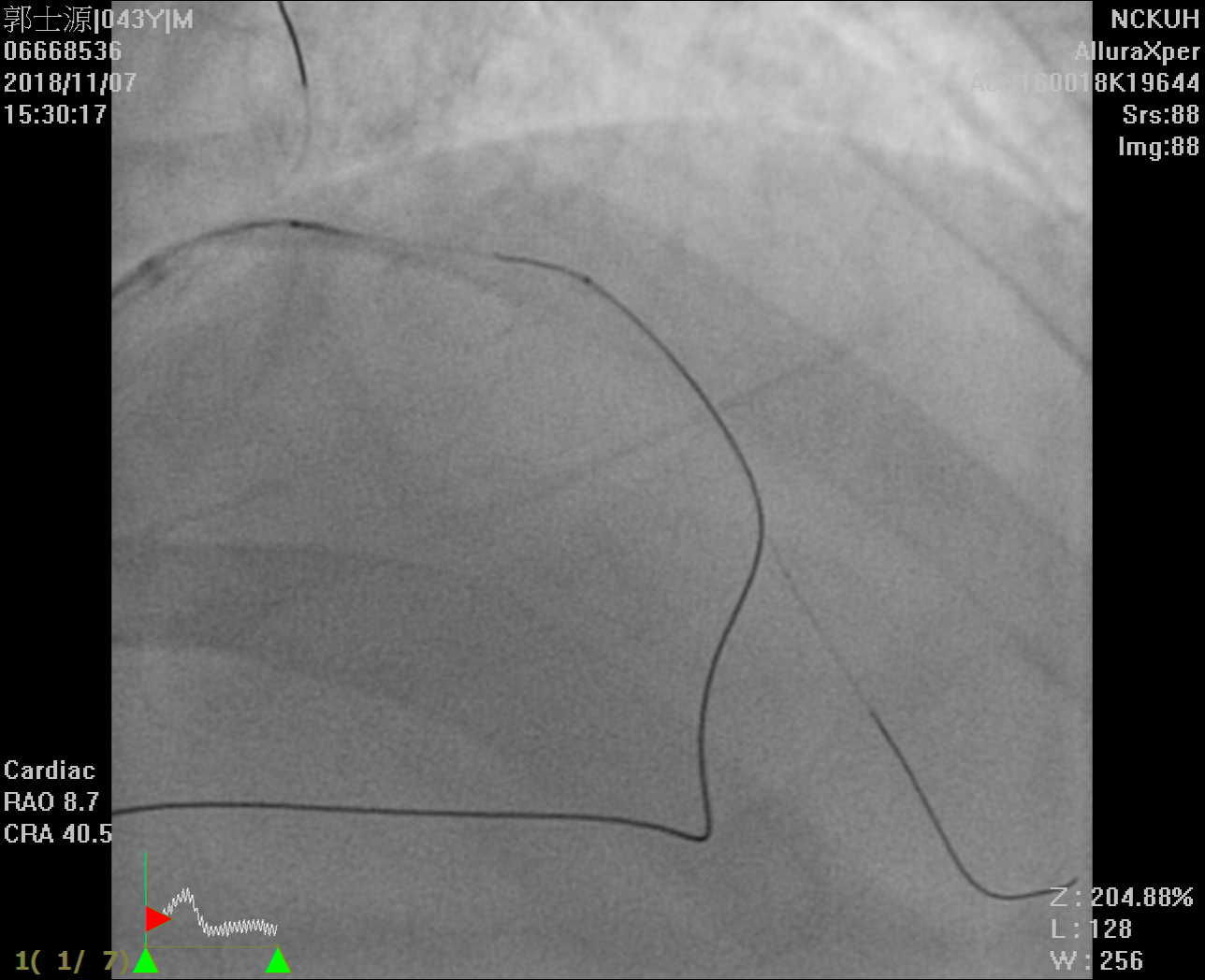  - Case Summary:
This is a case with LAD CTO with failedPCI. We re-tried with antegrade approach but was unable to make sure if thewire was in true lumen. Retrograde approach was indicated and we successfullypassed collateral channel. However, a longer microcatheter was not available sowe had to make a shorter guiding catheter to go on the procedure. When dealingwith CTO, sometimes crossing the total occluded part is not enough. Deviceissue is one of the obstacles. A home-made short guiding catheter may be thesolution in some circumstances.
|
|