Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191014_001
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| Perils of OCT in Recent Coronary Intervention | |
| Amitabh Yaduvanshi1, Mohan Nair2 | |
| Holy Family Hospital, India1, Max Heart & Vascular Institute, India2, | |
|
[Clinical Information]
- Patient initials or identifier number:
MK
-Relevant clinical history and physical exam:
60 years old malePresented to the emergency with retrosternal chest pain at rest of 4 hours duration.Smoker, diabetic on oral medicationsHaemodynamically stable, Maintaining SpO2 at room airFine basal crepts on chest auscultation
-Relevant test results prior to catheterization:
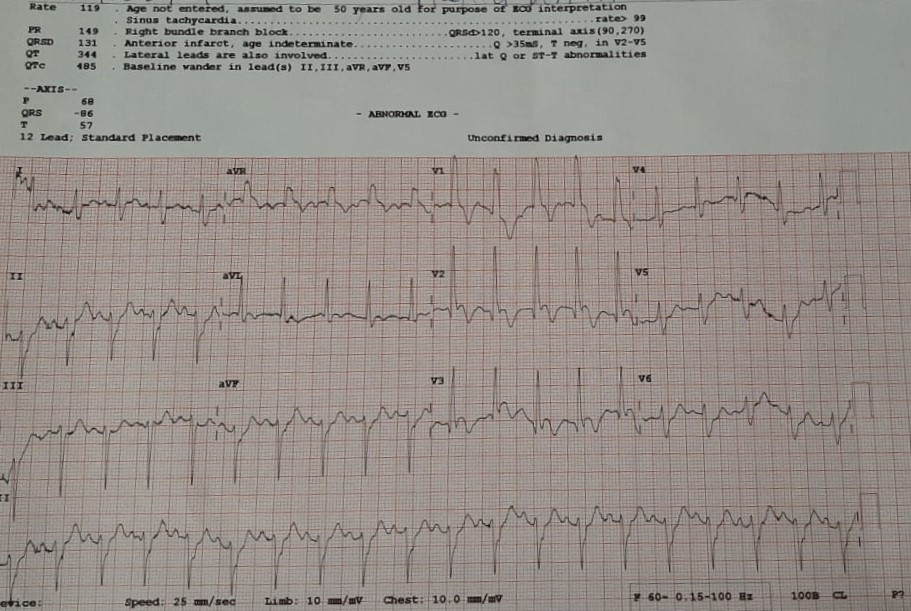
Electrocardiogram showed qRBBB with ST elevation in Anterior Leads.Troponin I was raised
 - Relevant catheterization findings:
Coronary Angiogram revealedLeft Anterior Descending Artery: Proximal 70% stenosis, mid 90% stenosisLeft Circumflex Artery: Distal 80% stenosis, OM2 proximal 70% stenosisRight Coronary Artery: Proximal 70% stenosis
|
|
|
[Interventional Management]
- Procedural step:
Primary Angioplasty to culprit vessel and staged PTCA to other vessel was planned.LAD lesion was crossed with BMW wire and the mid LAD lesion was dilated with 2.0 x 10mm balloon.A 3.0 x 40mm Orsiro stent was then deployed from ostial LAD up-to mid LAD at 14 atm. The stented segment was post dilated with 3.0 x 12mm non-compliant balloon at 18atm, TIMI III flow achieved
After 2 days patient was taken up for staged PTCA to LCx.There was a suspicion of stent under-expansion in LAD so OCT was planned.The LAD was crossed with a BMW wire and the OCT catheter was passed to distal LAD and OCT imaging run taken.It revealed good stent expansion and apposition in the distal stented segment however significant malapposition at the proximal stented segment, additionally it was detected that the wire had gone sub-stent in the proximal malapposed segment.Another BMW wire was taken for luminal entry however despite repeated attempts the wire couldn't be negotiated into the stent true lumen.Ultimately the proximal sub stent entry segment was crushed against the LAD wall with a 3.0 and 3.5mm balloon.Repeat OCT imaging showed suboptimal apposition of the crushed double layer of the stent but good luminal diameter and no dissection. Angiogram also revealed TIMI III flow.Angioplasty and stent implantation in LCx and the RCA was then done. - Case Summary:
Mild stent malapposition is common after angioplasty and inadvertent sub-stent passage of guide wire is possible on rewiring of these stents.
The profile of newer OCT catheters are so low that sub stent passage was not appreciated while introducing the catheter. It may be difficult to renegotiate the wire into true stent lumen if the stent is even mildly deformed. Crushing the stent against the vessel wall is a viable option in such cases with good immediate angiographic results. Significant malapposition still remained but may not have clinical significance as the patient has completed 3 months of event-free followup. |
|