Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191011_002
| CORONARY - Complications | |
| Misfortunes Never Come Singly - What I Met During a CTO PCI! | |
| Szu-Chi Chien1 | |
| Changhua Christian Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Y
-Relevant clinical history and physical exam:
He had hx of DM, and suffered resting chest tightness twice this year and began to feel exertional chest tightness since 14 days before. Radiation was noted to left shoulder and neck. No shortness of breath, nausea/vomitting, diarrhea, abdominal pain, dyuria, frequency or urgency. Due to the persisted symptoms stated above, he went to our CV OPD for further survey. At OPD, no cold sweating or chest pain were noted.
 -Relevant test results prior to catheterization:
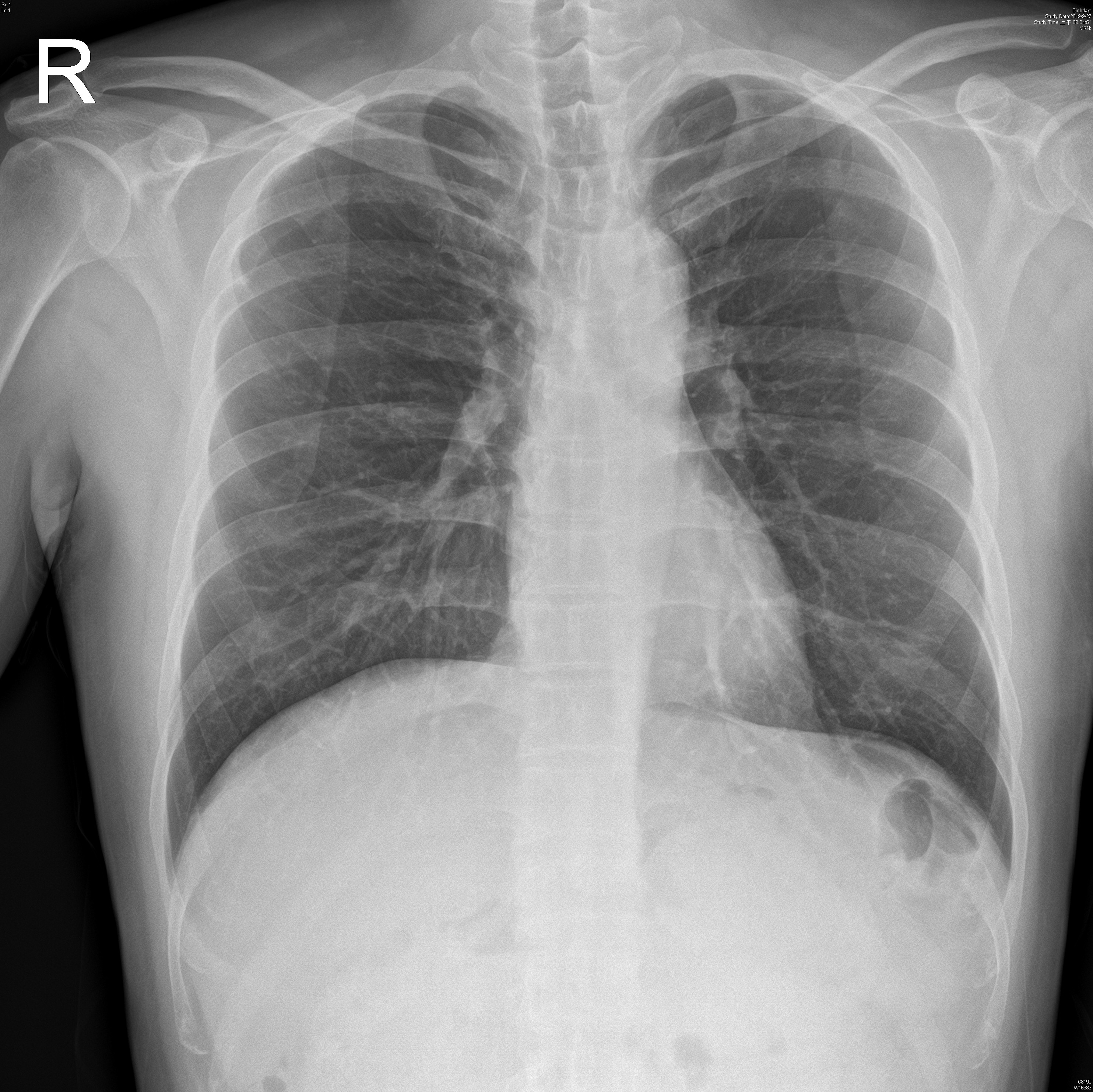
Cardiac enzyme elevation of Troponin-I: 0.52ECG showed non-specific changeCXR showed no obvious cardiomegalyEchocardiogram showed Regional wall motion abnormality, Hypolinesia: apex; middle-basal anterior, middle-basal lateral, middle-basal anteroseptal wall.
- Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
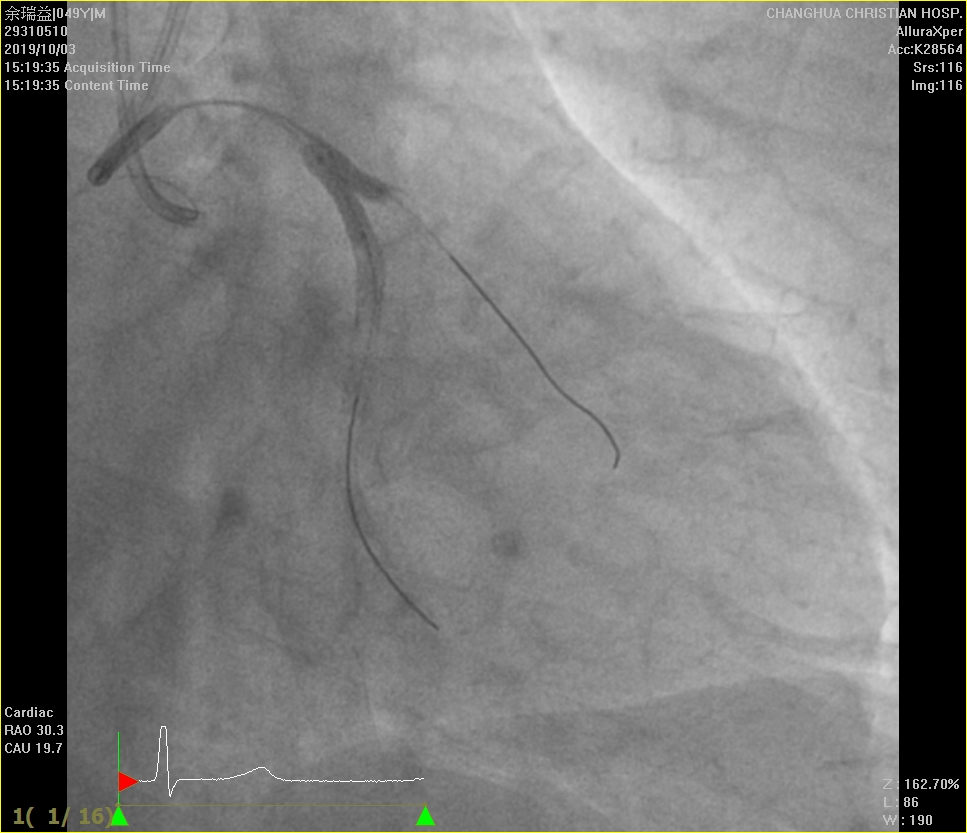
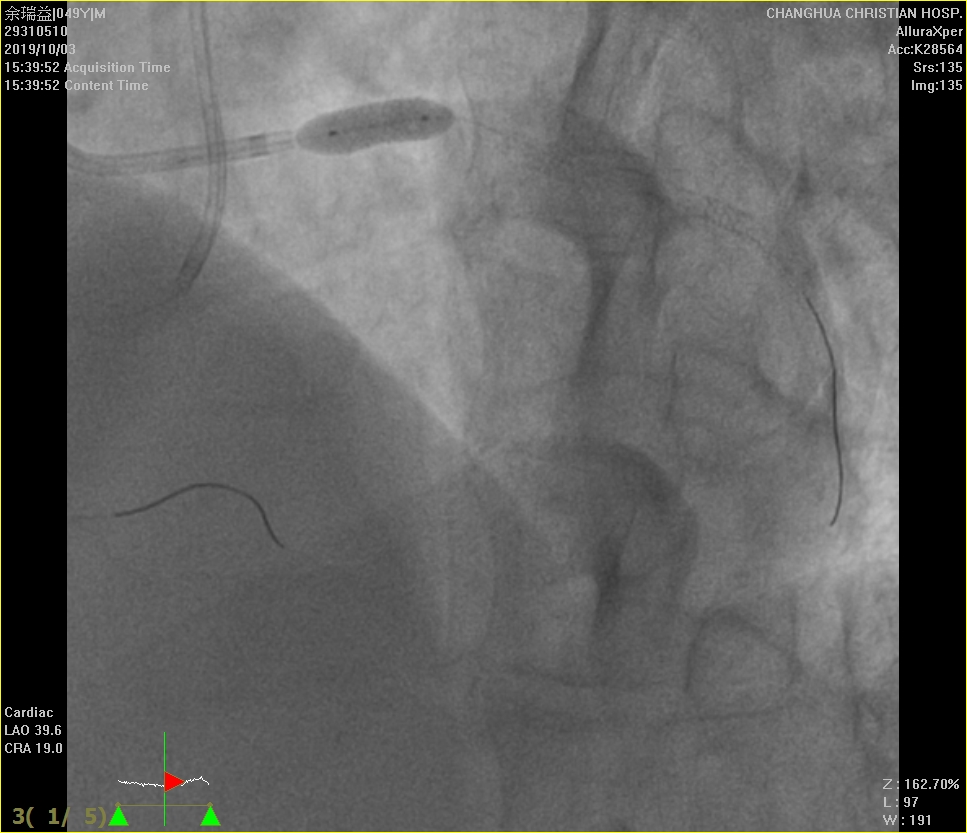
for LM, IVUS for LM optimization. Stent deployment with Resolute Onyx 5.0/12mm for LM.For LCX, apply Sion black wire to mid LCX with Codman 2.3Fr. MC via Launcher EBU 3.5SH/7Fr. guiding catheter, failed to advance to distal LCXThen apply sion black wire to OM as a guide, try UB 3 wire, but failed to advance to distal LCX due to tight lesion, step upto Progress 80 wire , successful puncture into mid LCX proximal cap, then wiring to distal LCX. Follow up contralateral CAG showed wire in the subintimal space. Parallel wire with Gaia 2nd, try to approach distal cap, but difficult to wiring. CAG showed RCA ostium dissection, suspected diagnositc catheter related. Exchange to Launcher JR 4/6Fr. guiding catheter, apply runthrough floppy wire carefully to distal PL. Bail-out stenting with Desyne X2 4.0/14mm inflated upto 14ATM. Wiring Progress 80 to reach distal cap of CTO , confimed by contral lateral angiogram. POBA with Sapphire 1.0/5mm for LCX, CAG showed jailed OM. Wiring with Sion black advace to OM, POBA with Sprinter 2.0/12mm inflated upto 10ATM for LCX. IVUS for confirmed true lumen: mid to distal LCX in subintiamal space, distal LCX in true lumen. Stent deployment for distal LCX with Resolute Onyx 2.5/38mm for distal LCX. Mini- crush technique to mid LCX to OM bifurcation lesion, Stent deployment for LCX to OM with Resolute Onyx 3.0/15mm , crushed by Resolute Onyx 3.0/34mm. KBT with NC TREK 3.0/15mm for LCX, TREK 2.75/12mm inflated upto 14ATM. IVUS showed stent well apposed
  - Case Summary:
CAD-3VD with LM lesion and LCX CTO c/w NSTEMI s/p successful PCI with POBA +stent deployment(DES*1) for distal LCX, LCX -OM bifurcation lesion(DES*2, mini-crush technique), POBA + stent deployment(DES*1) for LM. Bail-out stent deployment (DES*1) for RCA ostium disseciton induced by diagnostic catheter
|
|