Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191007_001
| CORONARY - Complications | |
| Trapped at Both Ends | |
| Hoong Sheng Loh1 | |
| National Heart Institute, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
MS
-Relevant clinical history and physical exam:
54-year-old male, an active smoker with coronary artery disease, hypertension and dyslipidemia was admitted for elective percutaneous coronary intervention to a chronic total occlusion in the ostial -proximal segment of left anterior descending artery. His blood pressure was 128/72 mmHg, heart rate was 68 beats per min and physical examination was unremarkable.
-Relevant test results prior to catheterization:
His resting ECG was normal with sinus rhythm. Chest X-ray was normal. Transthoracic echocardiogram showed normal left ventricular function with no regional wall motion abnormality.
 - Relevant catheterization findings:
A 3-week prior coronary angiogram showed a total occlusion in the ostial-proximal segment of left anterior descending artery with collaterals from distal right coronary artery and left circumflex artery. There were no significant disease in the left main, right coronary and left circumflex arteries.
|
|
|
[Interventional Management]
- Procedural step:
The left coronary system was engaged with 7F EBU 3.5 catheter via left radial artery and the RCA was engaged with 7F AL1 catheter via right femoral artery. The right iliac artery was tortuous. Bilateral contrast injection was performed to study the collaterals and we decided to attempt with antegrade approach first. The LAD CTO was easily crossed by Fielder XT-A wire with Caravel microcatheter. The wire was exchanged to a Runthrough Floppy wire and a BMW wire inserted into the left circumflex artery. The lesion was predilated with TREK 2.5 x 12mm up to 12 atm, stented with SYNERGY 3.5 x 24mm at 11 atm and postdilated with NC Emerge 3.5 x 15mm up to 20atm. The EBU catheter was removed first but we had difficulty to disengage AL1 catheter. After a few attempts, we realised the catheter was kinked and twisted in the iliac artery. We tried to disengage the catheter with a Amplatz goose neck snare 25mm but the catheter was deeply engaged into the RCA and the secondary curve of the catheter was sitting tightly in the aortic cusp. The goose neck snare failed to disengaged the AL1. Finally we reinserted the EBU with guidewire support, passed it below the primary curve of AL1 and successfully hooked it out from the RCA. Finally, the AL1 catheter was untwisted and removed from the femoral sheath.
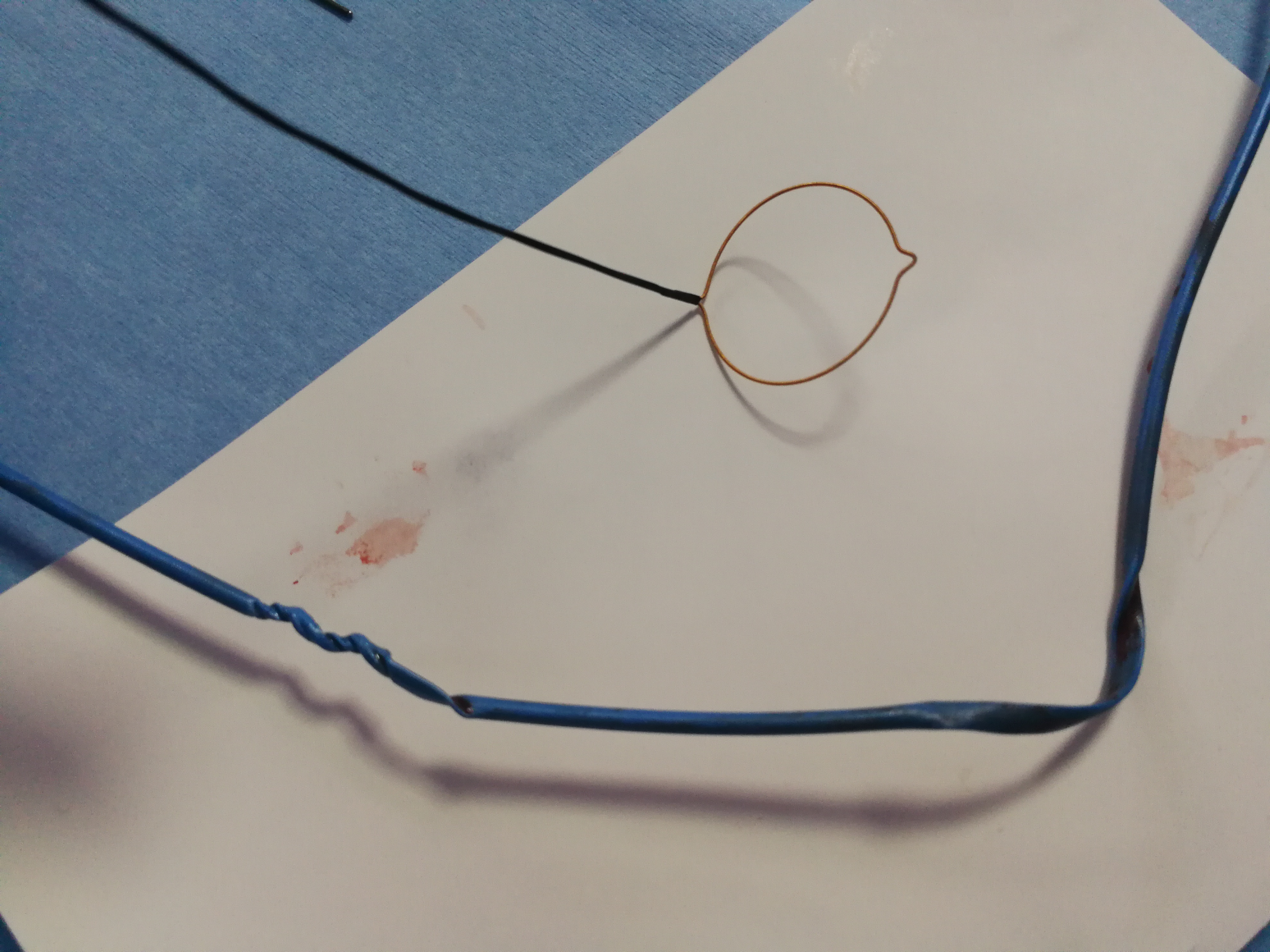 - Case Summary:
In this case, we have demonstrated the use of a EBU catheter to disengage an AL1 catheter that was twisted and deeply engaged into right coronary artery. The tortuous iliac artery and use of excessive force to manipulate the catheter might have caused the catheter to be twisted and kinked. This may be prevented using long femoral sheath to straighten the iliac artery before inserting the catheter and reinserting the catheter guidewire for better support before manipulating the catheter excessively.
|
|