Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191004_001
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Rotational Atherectomy in the Setting of an Acute Anterior Myocardial Infarction | |
| Rohith Stanislaus1, Mohamed Nazrul Mohamed Nazeeb1, Shaiful Azmi Yahaya1 | |
| National Heart Institute, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
MRAH
-Relevant clinical history and physical exam:
MRAH,a 57 year old gentleman with a past medical history of hypertension for close to 10 years presented with complaints of severe central crushing chest pain for 3 hours which was associated with diaphoresis. He did not complain of anyshortness of breath. Clinical examination on presentation was unremarkable and patient was hemodynamically stable with a blood pressure of 150/90mmHg and heart rate of 76bpm.
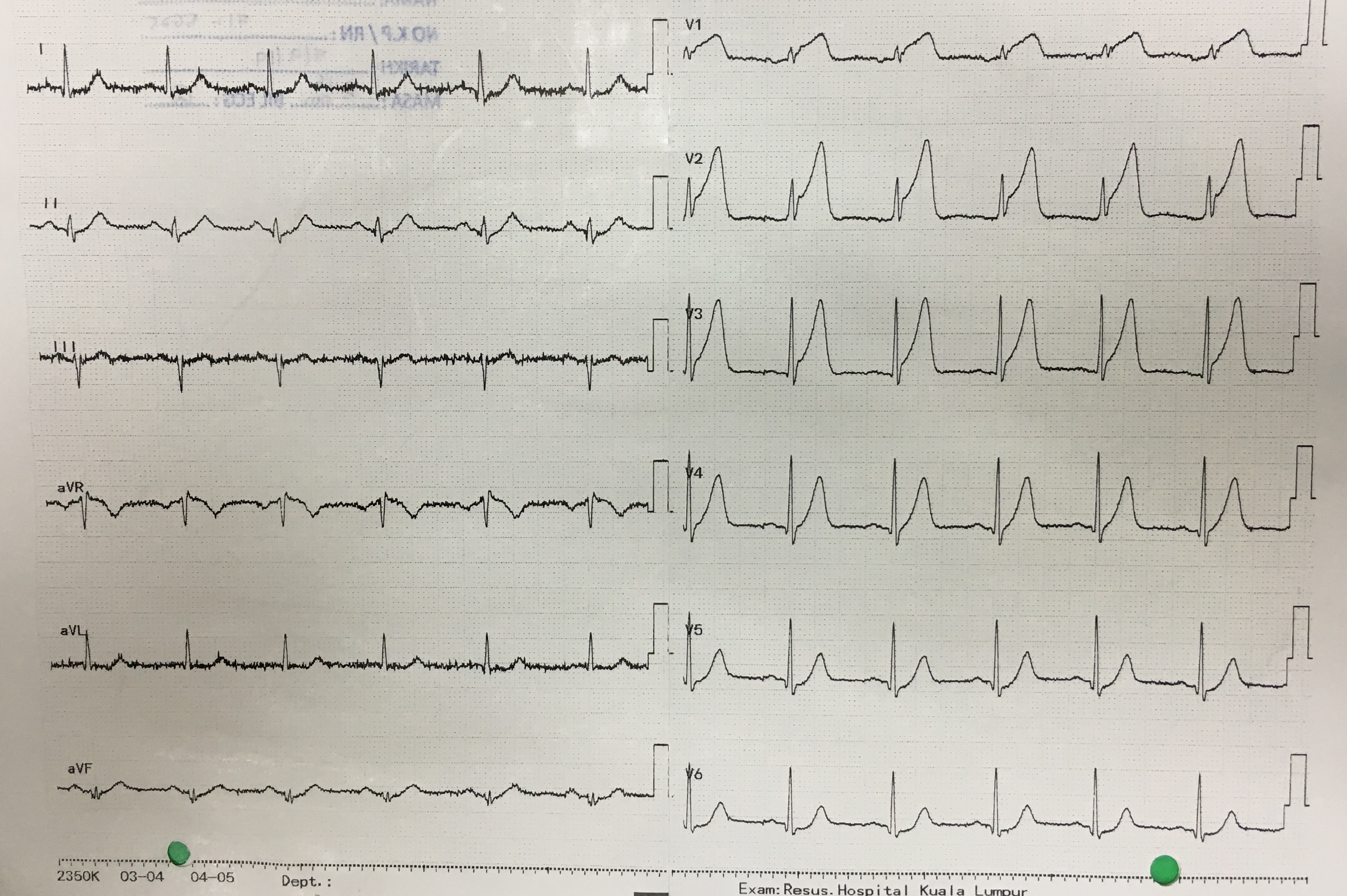
-Relevant test results prior to catheterization:
Patients ECG on presentation showed sinus rhythm with ST-segment elevation in leads v1-v3 with hyperacute T-waves in leads v4-v5. An Echocardiogram which was performed bedside at the emergency department prior to transfer to the Cath Lab showed an Ejection fraction of 50-55%,valves grossly normal, no evidence of any mechanical compromise and hypokinesia of the apex and septal wall. ECG and Echocardiogramchanges suggested a proximal LAD lesion. Blood results showed an elevated Trop T of 2888pg/ml
 - Relevant catheterization findings:
Patients ECG and Echocardiogramfindings suggested a proximal LAD lesion. A right radial approach using an Optitorque 5F to take diagnostic shots of the RCA showed mild stenosis of the proximal to mid-segment and severe stenosis at the proximal PL andPD branches. Then an EBU 3.5/6F guiding catheter for diagnostic shots/PCI to LAD. Left circumflex artery showed mild proximal stenosis and moderate stenosis of the proximal OM branch. The LAD showed severe stenosis proximal-mid segment with slow flow.
|
|
|
[Interventional Management]
- Procedural step:
Following COROS, we decided for PCI to LAD. Patient was given total 8000units of IA Heparin. Using an EBU 3.5/6F, we engaged the Left Coronary System. We used a RTF to cross the lesion. The wire crossed the lesion with relative ease. Initial plan was to pre-dilate the proximal to mid-segment with a semi-compliant WILMA 2.5/17mm balloon, however this balloon could not cross the lesion. We proceeded to use a smaller MINI TREK 1.5/15mm balloon, which also failed to cross the lesion. Then a smaller GENOSIS 1.0/5mm balloon was used and expanded to 18ATM. In spite of this pre-dilatation, the GENOSIS balloon was not able to cross the lesion. At this point, we had to make a decision regarding pursuing this lesion with rotational atherectomy. Thus a FINECROSS micro-catheter was used for wire exchange to a Rotawire. Rotablator 1.75 burr was attempted, which did not cross the lesion. Decided to change to a smaller 1.25burr which crossed the lesion. Following rotablation, noted dissection over the mid-LAD, thus we decided to pre-dilate further and then deploy stents. Predilatation was done using a WILMA 2.5/17mm balloon up to 12ATM from the mid-proximal LAD. Mid-LAD was stented with a ONYX 2.75/26mm at 18ATM then proximal-LAD was stented XIENCE 3.5/28mm at 16ATM. Then we proceeded to post-dilate from mid-LAD till the proximal segment with an NC EMERGE 3.5/15mm at 8-22ATM. Following PCI, noted good TIMI III flow down LAD with no immediate complications.
- Case Summary:
This is a case where Rotational Atherectomy was used successfully in the setting of an Acute Anterior Myocardial Infarction. Factors which contributed to its success was a patient who was hemodynamically stable throughout the procedure and early recognition that routine pre-dilation with semi and non-compliant balloons would not have been able to obtain satisfactory lesion preparation prior to stent deployment. It also highlights the possibility of using advanced techniques in the acute setting to achieve good angiographic results.
|
|