Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20190925_001
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| Large Burr Rotablation for Heavily Calcified Left Main and Ostial LAD Lesions | |
| Yi-Hsueh Liu1, Chun-Yuan Chu2 | |
| Kaohsiung Medical University Chung-Ho Memorial Hospital, Taiwan1, Kaohsiung Medical University Hospital, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Tu
-Relevant clinical history and physical exam:
This79-year-old female had the history of coronary artery disease post stenting in 2002, hypertension, type 2 diabetes mellitus, and old stroke. She presented with sudden onset of left chest pain without radiation for30 minutes. Her vital signs at emergency room were: E4V5M6, 37.1 ℃/ 110 bpm/ 16cpm, 181/70 mmHg, SpO2: 95 %. Physical examination showed tachycardia withoutobvious heart murmur.
-Relevant test results prior to catheterization:
Electrocardiogram revealed sinus tachycardia and T wave inversion in lead II, III, aVF, and V4-V6.
Laboratory findings demonstrated elevated cardiac enzyme (Troponin-I: 0.037->0.354->1.397ng/mL) Chest X-ray developed Cardiomegaly.  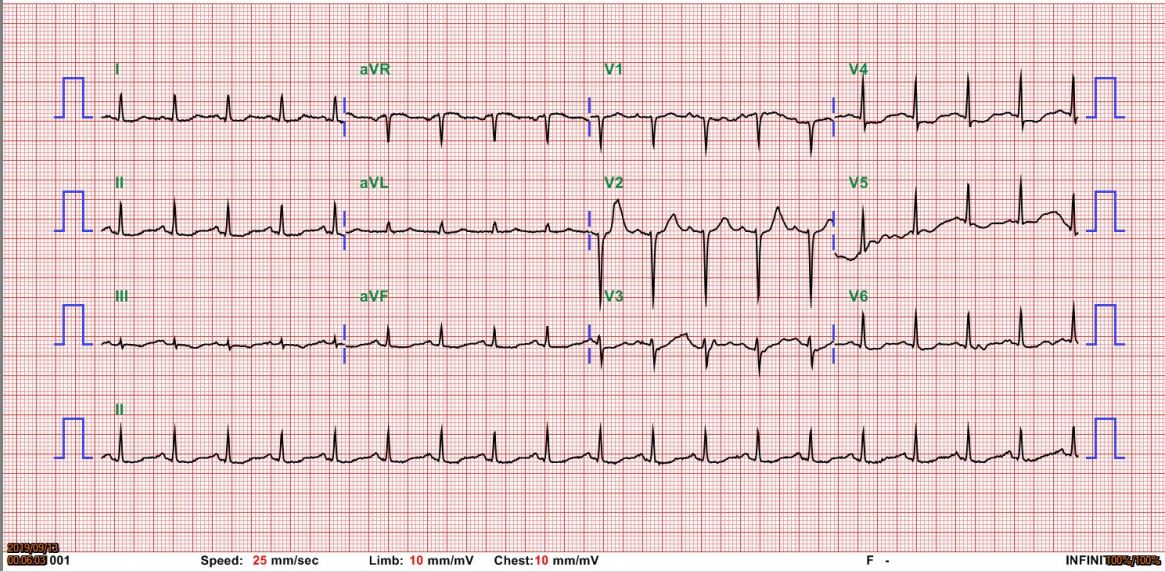 - Relevant catheterization findings:
Left main artery: 50%stenosis with calcification at bifurcationRight coronary artery:Segment 4 10% irregular stenosisLeft anterior descendingartery: Orifice 90% stenosis with calcification Segment 6 50-70% stenosisLeft circumflex artery: nosignificant stenosis
|
|
|
[Interventional Management]
- Procedural step:
1. A 7 Fr sheath was inserted thorough right femoral artery
2. Coronary angiogram showed heavily calcified Left main and Ostial LAD Lesions 3. Guiding catheter: EBU 3.5 Side hole 7F engaged to LCA 4. IVUS showed calcified plaque between Left main and ostial LAD (270 to 360 degree in circumference) with decreased luminal area. 5. Guide wire: Runthrough floppy, advanced to LAD smoothly, then change to RotaWire Extra Support with MINI TREK II OTW 1.5X6mm balloon support;Sion blue ES, advanced to LAD D16.Rotablation:Rotablation using a 1.75 mm burr was performed at a speed of 150,000 r/min. The burr encountered some transient friction during the course of LM-LAD but finally the burr advanced just before the original LAD stent. 7.Balloon angioplasty for LAD and LAD D1 -KBT (Kissing balloon angioplasty) --Maverick balloon 2.0x20 mm, dilated at LAD D1 with 10-12 atm --NC Emerge balloon 2.75x12 mm, dilated at LAD with 10-12 atm 8. Stent: XIENCE Alpine (Drug-eluting stent) 2.75x28mm, deployed at LM-LAD with 10-12 atm 9. Post-dilatation: -Accuforce balloon 3.0x15 mm, dilated up to 8-16 atm for 4 times 10 . Balloon angioplasty for LM-LAD and LM-LCX KBT (Kissing balloon angioplasty) --Accuforce balloon 4.0x8 mm, dilated at LM-LAD up to 8 atm --Accuforce balloon 2.5x15 mm, dilated at LM-LCX up to 8 atm 11. Proximal optimisation technique (POT): Accuforce balloon 4.0x8 mm, dilated at LM up to 12-16 atm for 2 times 12. Final angiography: good result with TIMI 3 flow - Case Summary:
Rotational atherectomy is auseful adjunctive device in interventional treatment of heavily calcifiedcoronary arteries. We initially used RotaExtra Support Wire accompany with single 1.75mm large burr as the initial debulking strategy for heavily calcified LM-ostial LAD plaque. Rotationalatherectomy allowed for substantial plague modification that further successfulstent deployment with good apposition and expansion.
|
|