Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20190918_004
| CORONARY - Complications | |
| Retrieve Methods of the Rotablator Burr Entrapment | |
| Tse-Husan Yang1, Feng Yu Kuo1, Wei-Chun Huang1, Guang-Yuan Mar1 | |
| Kaohsiung Veterans General Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
6748932
-Relevant clinical history and physical exam:
82 year old man has underlying disease : hypertension, CAD, TVD s/p PTCA and DES placement for 10 years. He had chest tightness and general weakness since this morning, and condition did not improve after taking NTG tablet.
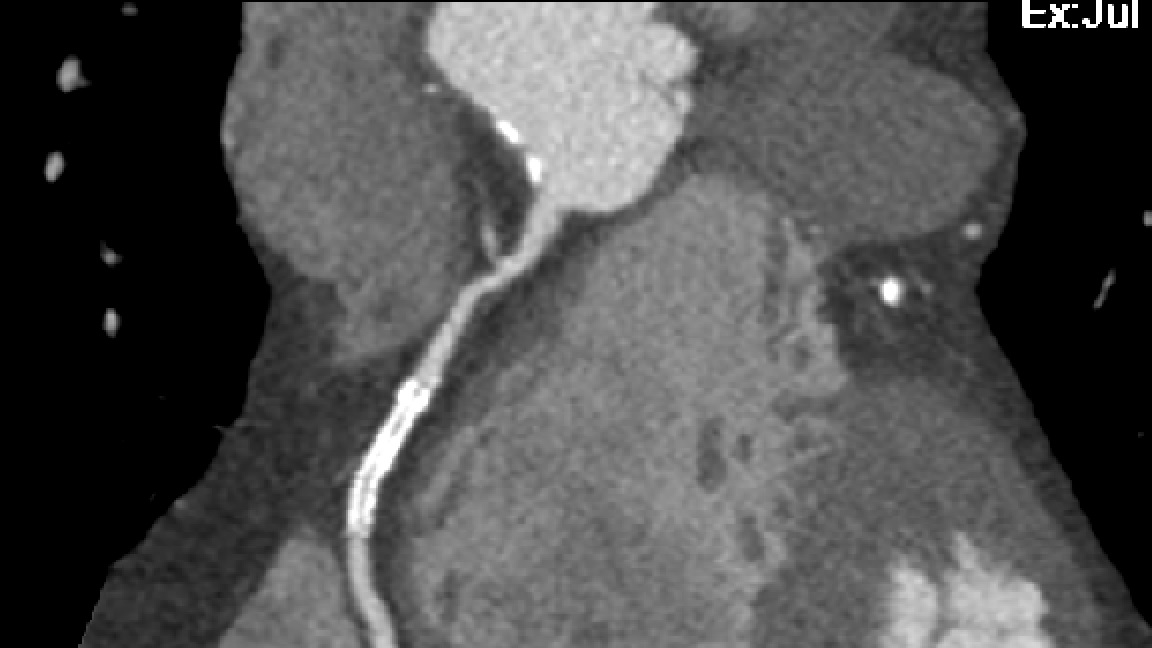
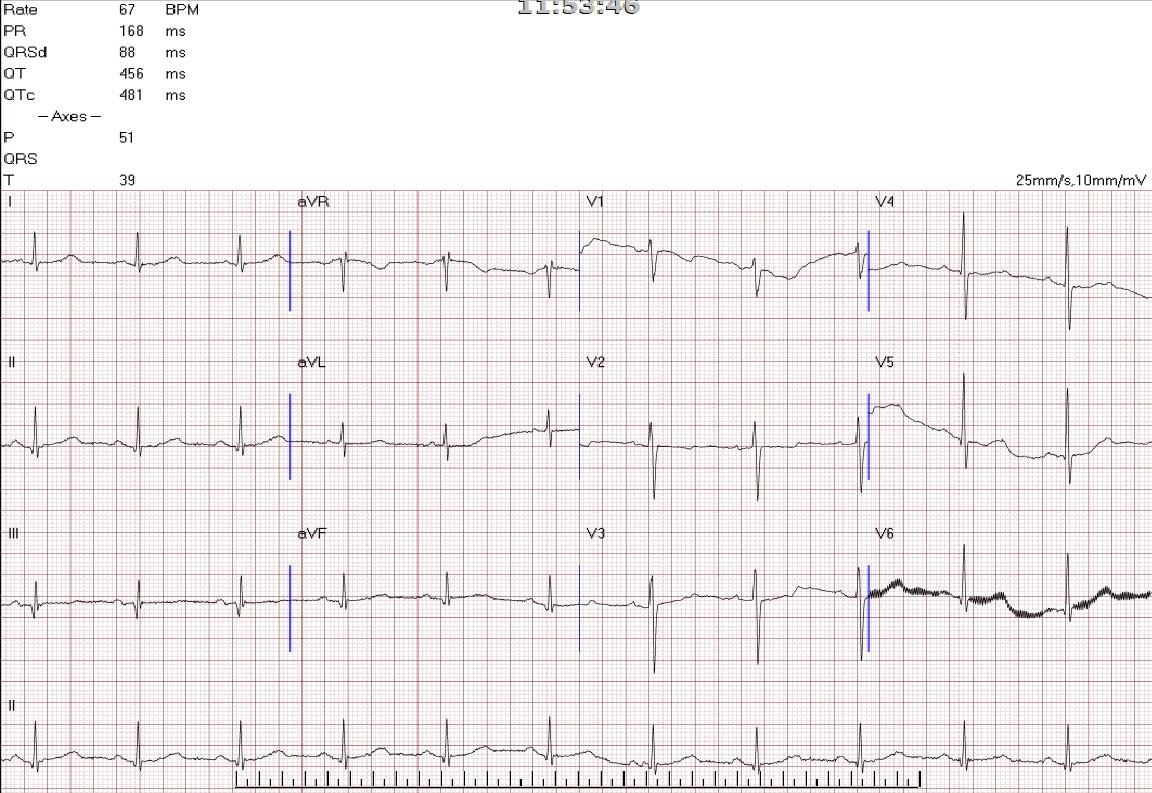 -Relevant test results prior to catheterization:
CT-Angiogram Coronary revealed triple vessel disease with recurrent significant stenosis over RCA-D. LAD-M
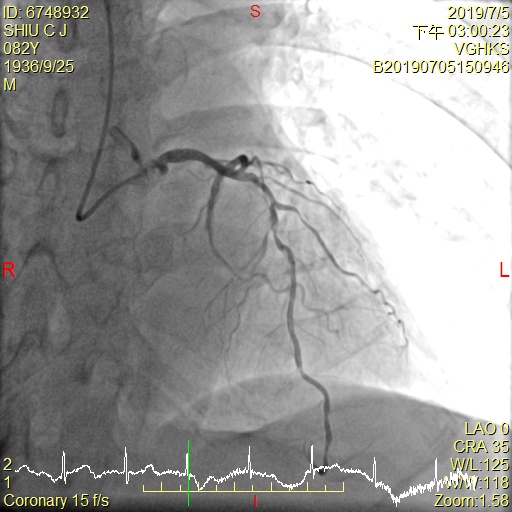
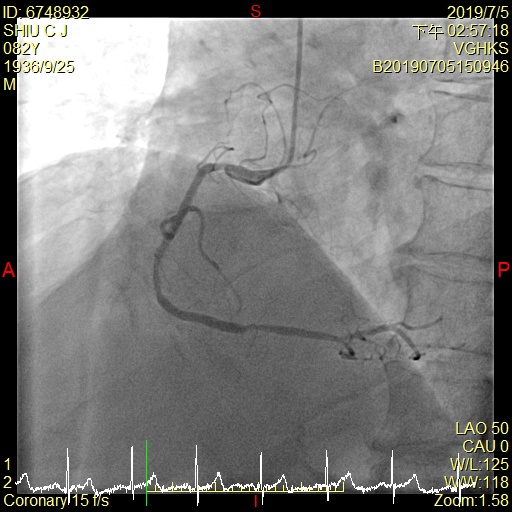
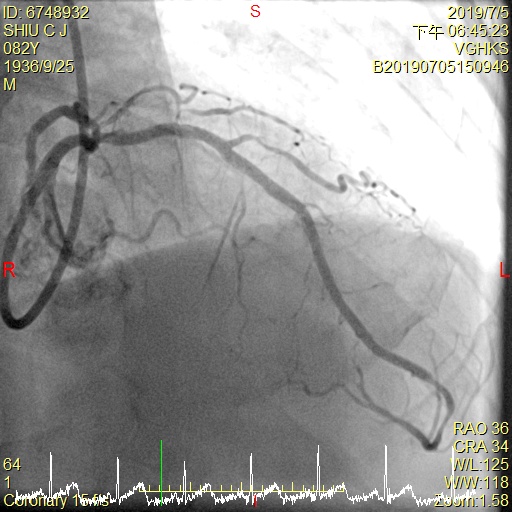
  - Relevant catheterization findings:
LAD: -P to M: calcification, 60% stenosis -D: heavy calcification, critical stenosis 90%LCx: -M: 60-70% stenosis -D: s/p stenting, no significant instent restenosisRCA: -M: s/p stenting, 40-50% instent restenosis -D: 70% stenosis
  |
|
|
[Interventional Management]
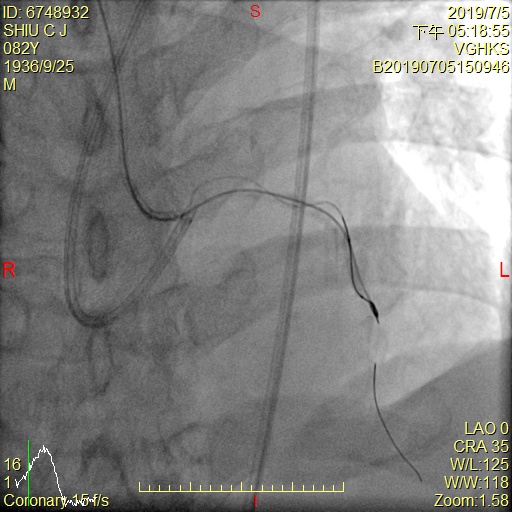
- Procedural step:
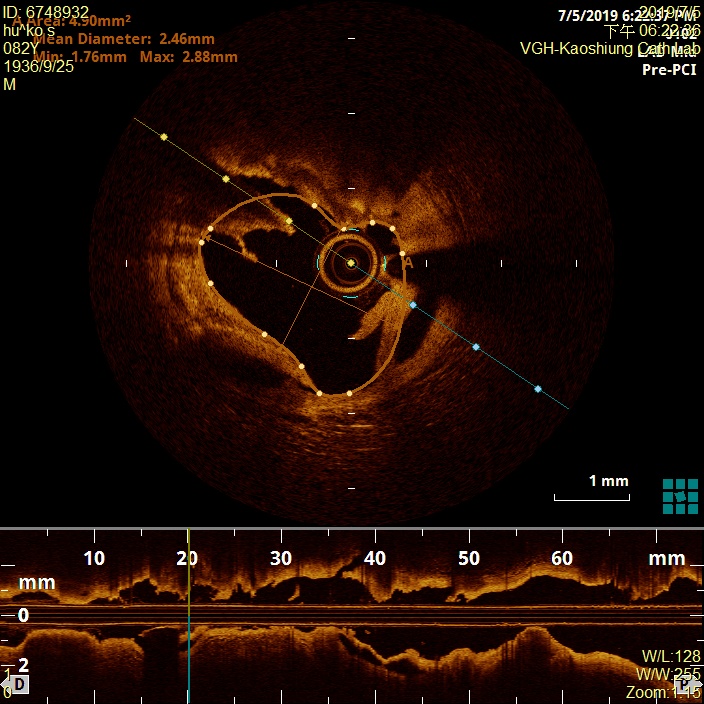
LCA was engaged by a 3.5mmX6F Ikari Guide catheter from R't radial artery. LAD was crossed by a Sion 0.014" 180cm Guidewire; for hardly cross distal LAD, we changed to Fielder XT-A 0.014" 190 cm Guidewire, assisted by a 1.5X20 mm Balloon, which was inflated over LAD-M to D lesion. However, OCT could not pass. We tried to pass a 2.0X20 mm Balloon but failed, even assisted by a 5.5Fr GuideLiner Microcatheter. We use two1.0x8mm balloon to dilated the lesion and the balloon busted while inflation. Therefore Rotablation with 1.25 burr was performed. Unfortunately, the burr entrapped into the distal lesion, We tried to pull back trapped RotaBurr by insertion a 5.5Fr GuideLiner Microcatheter and ST01 Microcatheter but in vain. .A 1.0X8mm Balloon, 2.0X15mm Trek Balloon, and a 2.5X15mm Trek Balloon was repeatedly inflated over LAD-M to D. We pulled back the rotaburr eventually, and the entrapment was resolved. OCT showing diffuse and spiral dissection. We deployed stent and the peocedure was finished with TIMI: 3 flow.
   - Case Summary:
Rotablator-burr entrapment is the a serious complication while performed the procedure, especially when we dealing with calcified lesion. Even with 1.25mm burr still could happen. This case demonstrated how to resolved this situation via step by step useful technique.
|
|