Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20190918_002
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Acute Coronary Embolism Presenting as STEMI During BMV Procedure | |
| Ahmad Pandu Pratama1, Arwin Saleh Mangkuanom2, Amir Aziz Alkatiri2, Doni Firman2, Sunarya Soerianata3, Nur Haryono4 | |
| Mohammad Hoesin General Hospital, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2, Pondok Indah Hospital, Indonesia3, ISIC, Indonesia4, | |
|
[Clinical Information]
- Patient initials or identifier number:
LA
-Relevant clinical history and physical exam:
40-year-old male with severe MS came to NCCHK for elective BMV. BMV was decided by surgical conference since it was considered beneficial due to surgery deemed very high risk. He felt dyspnea on effort, with no orthopnea or chest pain. Warfarin was discontinued 4 days priorOn physical examination, PSM grade 3/6 at best heard at LLSB and MDM grade 2/4 best heard at apexDuring left ventriculography, MR sellers grade III was found and coroangiography was performed since surgery was indicated
-Relevant test results prior to catheterization:
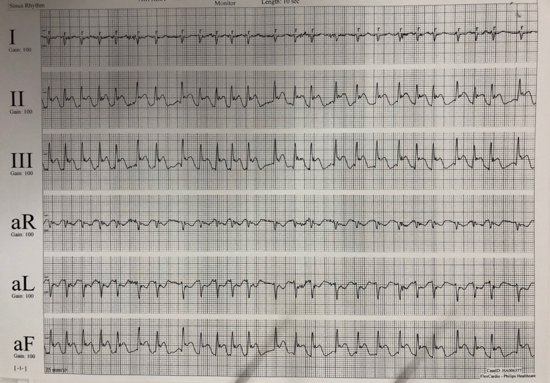
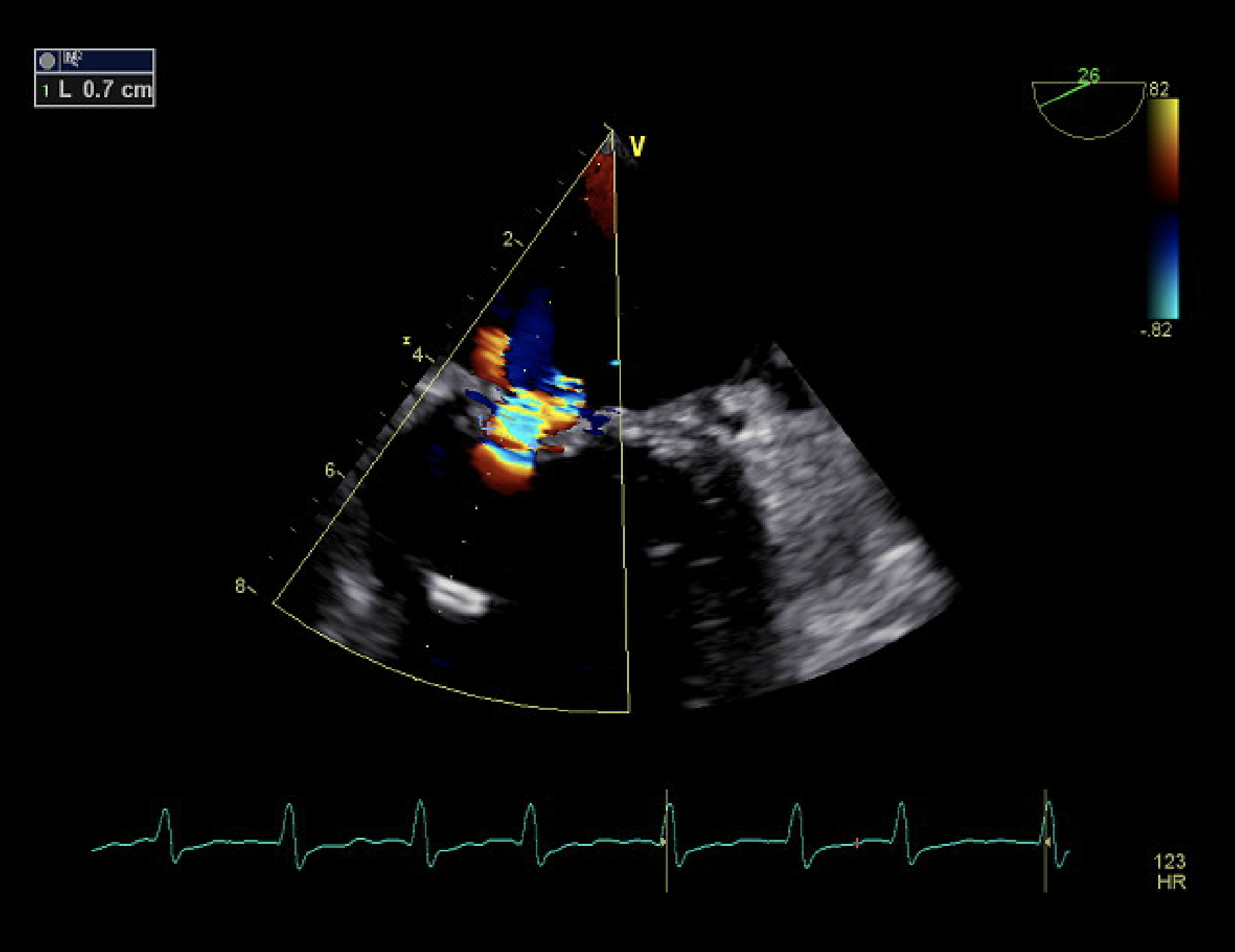
ECG before BMV: Atrial fibrillation (AF), HR 70 bpm, right axis deviation, QRS duration 0,10s, RVHLab:Hemoglobin 15.5g/dL, Platelet 249.000/μL, PT 15.4s, INR 1.30, Creatinine 1.02 mg/dLTEE before procedure:Severe MS, AML PML thickened (1); calcified (2), chordae fused (2), MVA 0.6cm2 (planimetry), mMVG 8 mmHg, LVEF 54%, TAPSE 1.8cm, no LA and LAA thrombus, SEC at LA and LAAECG during coroangiography: AF with ST elevation at lead II, III, aVF
   - Relevant catheterization findings:
Left Ventriculography graphy,:leaftlets appeared dooming in diastole, tampak MR Sellers grade III. Dari TEE, didapatkan moderate MR (VC 0.7 cm, jet sangat eksentrik ke posterior) dan severe TR (uncoapted leaflets)Coroangiography:LM : NormalLAD : Slow flow, thrombus (+), total oklusi di distal LADLCx : Slow flow, thrombus (+), total oklusi di distal LCxRCA : Normal
|
|
|
[Interventional Management]
- Procedural step:
- Case Summary:
Acute Myocardial Infarction (AMI) due to Coronary Embolism (CE) is a rare yet an under-diagnosed phenomenon and represent a high-risk subgroup of MI. 10% of AF patient with CE developed recurrent episode when INR is inadequate (mean 1.47). Based on current evidence, proper risk stratification and the use of anti-platelet aggregation, anticoagulants and thrombus aspiration could be the optimal treatment strategy
|
|