Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
ABS20200616_0001
| Complications | |
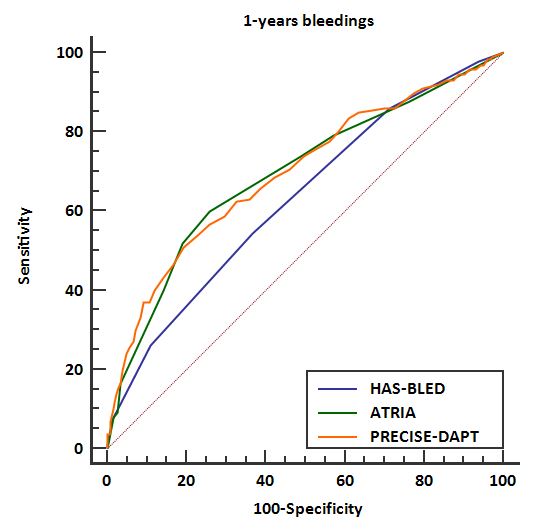
| Performance of the HAS-BLED, ATRIA, and PRECISE-DAPT Bleeding Risk Scores in Atrial Fibrillation Patients Using Antiplatelet Agents or Oral Anticoagulants | |
| Sun Young Choi1, Guangxi Yuan2, Moo Hyun Kim3, Kwang-Min Lee1 | |
| Dong-A University Medical Center, Korea (Republic of)1, DONG-A University Hospital, China2, Dong-A University Hospital, Korea (Republic of)3 | |
|
Background:
Various bleeding risk scores have been proposed to assess the risk of bleeding inatrial fibrillation (AF) patients undergoing anticoagulation. PRECISE DAPTscore has been developed to assess the out-of hospital bleeding risk inpatients receiving dual antiplatelet therapy (DAPT). Our objective was to comparethe predictive performance between the HAS-BLED (Hypertension, AbnormalRenal/Liver Function, Stroke, Bleeding History or Predisposition, LabileInternational Normalized Ratio, Elderly, Drugs/Alcohol), ATRIA (Anticoagulationand Risk Factors in Atrial Fibrillation), and PRECISE-DAPT (Predicting BleedingComplication in Patients Undergoing Stent Implantation and Subsequent DualAntiplatelet therapy) score in AF patients using antiplatelet agents or anticoagulants.
|
|
|
Methods:
We recruited 1,114consecutive AF patients (51% male; median age, 71 years) receiving antiplateletagents or oral anticoagulants from January 2014 through December 2018. The HAS-BLED, ATRIA, and PRECISE-DAPT bleeding risk scores were calculated from patients’ clinical characteristics. Majorbleeding was defined as according to the Bleeding Academic Research Consortium(BARC) criteria (type 3 or 5: hemodynamic instability, need for transfusion,drop in hemoglobin ≥ 3 g, and intracranial, intraocular or fatal bleeding). Theperformance of risk scores were assessed by C-statistic.
|
|
|
Results:
Bleeding events occurred in 72 patients (6.5%) from 30 days till1-year follow-up. Based on the C-statistic, PRECISE-DAPT score (AUC: 0.70, 95%CI: 0.67-0.72) and ATRIA score (AUC: 0.69, 95% CI: 0.66-0.72) had a good performance, significantly better than HAS-BLED (AUC:0.64, 95% CI: 0.61-0.67) (p = 0.03). And, PRECISE-DAPT score was similar to ATRIA score in predicting bleeding events.
 |
|
|
Conclusion:
All 3 bleeding risk scores demonstrated onlymodest performance in predicting 12-month bleedings in Korean AF patientsreceiving antiplatelet agents or oral anticoagulant (warfain or NOAC), althoughthe predictive ability of HAS-BLED score was not superior to ATRIA, andPRECISE-DAPT scores. PRECISE-DAPT score for DAPT can be used as bleeding riskscore in AF patients with HAS-BLED, ATRIA and PRECISE-DAPT score.
|
|