Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
ABS20191115_0021
| Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Is Door to Balloon(D2B) Time Still Important in ST Elevation Myocardial Infarction (STEMI) Patients? | |
| Moo Hyun Kim1, Kwang-Min Lee2, XUAN JIN1 | |
| Dong-A University Hospital, Korea (Republic of)1, Dong-A University Medical Center, Korea (Republic of)2 | |
|
Background:
Guidelines for the treatment of ST-segment elevation myocardial infarction recommend a door-to-balloon time of 90 minutes or less for patients undergoing primary percutaneous coronary intervention (PCI). However, it is not well known whether there are further differences present within D2B time < 90 minutes
|
|
|
Methods:
From the Korean Registry of Regional Cardiocerebrovascular Center for Acute Myocardial Infarction (July 2016 - Sept 2018), patients over 18 years old who were performed primary PCI in STEMI patients were selected. We compared in-hospital event (all-cause death, cardiac arrest, CVA, bleeding) according to D2B time <60, 60~90, >90 minutes. We also calculated the receiver operator characteristic (ROC) curve for door to balloon time in the prediction of In-hospital event and defined the optimal cut-point value.
|
|
|
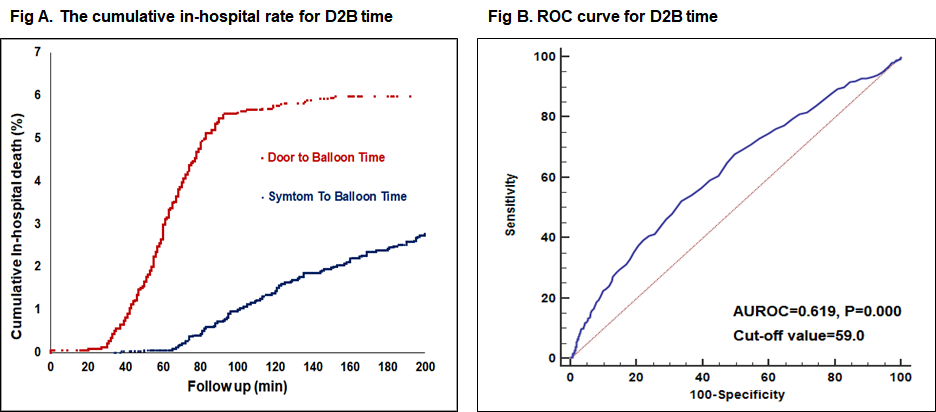
Results:
In terms of the in-hospital death rate according to D2B, the in-hospital death rate of D2B has increased significantly from 30 minutes or more. The AUC values for in-hospital event were 0.619, respectively. Optimal cutoff scores of in-hospital evet were 59, respectively (fig A, B). Therefore, we defined the cut-point for D2B time as <60min, 60~<90min, ≥ 90min. Compared to D2B time<60min, 60min ≤ D2B time <90min, D2B time≥60 minutes was associated with increased risk of mortality (4.1% vs. 8.7% vs. 18.6%; p<0.001), cardiac arrest (5.8% vs. 11.0% vs. 20.2; p<0.001), CVA (0.4% vs. 1.1% vs. 4.7; p=0.002). As a result of logistic regression analysis, in-hospital death of D2B time 90 min was 3.6 times higher than D2B 60 min(OR: 3.639, 95% CI: 2.014 - 6.577), and arrest of D2B time 90 min was 2.9 times higher(OR: 2.955, 95% CI: 1.693 - 5.158) and CVA of D2B time 90 min was 12.0 times higher(OR: 12.041, 95% CI: 4.030 - 35.979) than 60 minutes(Table 1).
 |
|
|
Conclusion:
In patients who had ST-segment Elevation Myocardial Infarction, the balloon time <60 minutes is associated with favorable outcomes. These data suggest that additional strategies are needed to reduce in-hospital mortality in this population.
|
|